Leukocytosis in penetrating trauma (abdominal and osseous/thoracic): a cross sectional study in Juárez, México
Juan de Dios Díaz-Rosales MD, MSc.1*, Lenin Enríquez-Domínguez MD.2*, Baltazar Aguayo-Muñoz MD.3*, Jesús E. Romo-Martínez MD4*, Beatriz Díaz-Apodaca MD, PhD.5*
1* Professor. Health Sciences Department / Universidad Autónoma de Ciudad Juárez, México. Calle Tlaxcala 3020-4. PRONAF. Ciudad Juárez. México. Teléfono: (656) 4410541. E-mail: jdedios.uacj@gmail.com
2* General Surgeon / Surgery Service - Hospital General de Ciudad Juárez / Universidad Autónoma de Chihuahua. México. E-mail: lenin_enriquez@hotmail.com
3* General Surgeon / Surgery Service - Hospital General de Ciudad Juárez / Universidad Autónoma de Ciudad Juárez. México. E-mail: al127920@alumnos.uacj.mx
4* Epidemiologist. Biostatistics and Epidemiology Department / Hospital General de Zona No. 11. Ciudad Delicias. México. E-mail: jesus.romom2@imss.gob.mx
5* Professor. Health Sciences Department / Universidad Autónoma de Ciudad Juárez, México. E-mail: bdiaz@uacj.mx
Archivos de Medicina (Manizales), Volumen 15 N° 2, Julio-Diciembre 2015, ISSN versión impresa 1657-320X, ISSN versión en línea 2339-3874. Díaz Rosales J.D.; Enríquez Domínguez L.; Aguayo Muñoz B.; Romo Mrtínez J.E.; Díaz Apodaca B.
Recibido para publicación: 23-05-2015 - Versión corregida: 26-08-2015 - Aprobado para publicación: 10-11-2015
Summary
Objective: the objective of this study is to compare white blood cells (WBC) count in patients with penetrating abdominal trauma isolated and associated with osseous and/or thoracic injury. Material and methods: cross-sectional study that compares the WBC count as factor associated with major injury in two groups of patients with abdominal penetrating trauma; group patients with penetrating abdominal trauma isolated (PATI) versus group patients with penetrating abdominal trauma associated with osseous and or thoracic injury (PAT/OT). Results: one hundred and eighty six patients are included. Ninety five (87.2%) patients in PATI group have leukocytosis vs 67 (87%) patients in PAT/OT have leukocytosis. The mean of WBC for PATI group is 14,200 per mm3 (±3.500); whereas, whereas the mean of WBC for PAT/OT group is 16,400 per mm3 (±4.700). This study shown a statistically significance difference in mean of leukocytosis between groups (p=0.01). Conclusion: a significant elevation of WBC count in patients with PAT/OT is observed in comparison with PATI patients.
Key Words: leukocytosis, leukocyte Count, abdominal Injuries, wounds, penetrating.
Díaz-Rosales JD, Enríquez-Dominguez L, Aguayo-Muñoz B, Romo-Martínez JE, Díaz-Apodaca B. LeukoCytosis in penetrating trauma (abdominal and osseous/thoracic): a Cross seCtional study in Juárez, México. Arch Med (Manizales) 2015; 15(2):220-5.
Leucocitosis en trauma penetrante (abdominal vs torácico/óseo): estudio transversal en Ciudad Juárez, México
Resumen
Objetivo: el objetivo de este estudio es comparar el nivel de leucocitos en pacientes con trauma abdominal penetrante aislado y asociado a trauma óseo y/o torácico. Materiales y métodos: estudio analítico y transversal que compara dos grupos de pacientes con trauma abdominal penetrante; un grupo con trauma abdominal penetrante aislado (TPAA) y el otro grupo con trauma abdominal penetrante asociado a trauma óseo y/o torácico (TPA/OT). Se examina si el promedio de leucocitos entre los dos grupos está asociado a una mayor lesión. Resultados: ciento ochenta y seis pacietnes fueron estudiados, no se observó diferencia en la proporción de pacientes que sufrieron de leucocitosis entre los grupos. Sin embargo, en los promedios de leucocitos si existe una diferencia estadísticamente significativa (14,200 vs 16,400 per mm3 ; p = 0.01) en el promedio de leucocitos entre los dos grupos, a favor del grupo con TPA/OT. Conclusiones: una elevación significativa del promedio de leucocitos en pacientes con TPA/OT es observada en comparación con el grupo de pacientes con TPAA y esto traduce en una mayor respuesta inflamatoria.
Palabras clave: leucocitosis. recuento de Leucocitos. traumatismos abdominales. heridas penetrantes.
Introduction
Penetrating abdominal trauma (PAT) affects approximately 35% of patients admitted to urban trauma centers in United States1. The abdominal trauma is an important cause of morbidity and mortality, abdomen is the third lead zone of human anatomy affected by traumatism that require surgery (20%) and hospitalization (90%)2.
The evaluation of PAT aims to identify patients who need operation to prevent submitting them to the risks of unnecessary surgical procedures. It is still debated whether the examination is reliable or additional tests should be routinely ordered. Identifying significant injury - in trauma patients - with early markers of injury could aid the physical, anamnesis, and other tests in detecting and/or measuring severe injury in penetrating trauma victims.
Major injury is associated with a major stress-induced neurohumoral response to stimulate the secretion of epinephrine and cortisol, these stress-induced hormones produce leukocytosis from both bone marrow and splenic sources3. Leukocytosis is defined as a white blood cells (WBC) count greater than 11,000 per mm3 (11 ×109 per L)4. Leukocytosis in trauma or stress is due to neutrophilia, caused by neutrophil margination, and not to increase bone marrow production or releases immature cells or bands5. During normal circumstances, estimated life span of WBC is 11 to 16 days, in inflammation states this phenomenon is short-lived though, lasting only minutes to a few hours, at which time apoptosis occurs6.
There are few studies that compare levels of leukocytes in patients with abdominal trauma3,5,7. Therefore, WBC count could serve as an easy-to-obtain early marker for serious injury4,5,8,9. The hypothesis is that patients with significant injury should have higher levels of leukocytosis compared to patients with minor injuries. The objective of this study is compare the WBC count in patients with PAT isolated (PATI) versus patients with PAT associated with osseous and/or thoracic injury (PAT/OT).
Materials and methods
This is a cross sectional and analytic study that is conducted at Hospital General de Ciudad Juárez (HGCJ), a Second Health Care Level Hospital, in Juárez (México). The local institutional review board of Universidad Autónoma de Ciudad Juárez and HGCJ reviewed and approved this study according to bioethics statutes (NOM-012-SSA3-2012).
Entry criteria included patients aged over 14 years old and under 50 years old; with abdominal gunshot trauma isolated and associated with osseous and/or thoracic injury; treated with therapeutic laparotomy; and admitted from April 1, 2008 to December 31, 2010. Exclude criteria included hemodynamically instability, non-gunshot penetrating abdominal trauma (e.g., stab wound trauma), lack of WBC count on admission, and early or late death by morbidity related to trauma.
Patients are divided into two groups: patients with PATI (group I) versus patients with PAT/OT (Group II). Data collected are: age, gender, period of time from trauma to hospitalization, drugs or alcohol intoxication, associated osseous or thoracic injuries, intra-abdominal organs injured, preoperative WBC count, preoperative level of neutrophilia, preoperative level of hemoglobin, preoperative level of hematocrit, and hospital stay. Variables measured in nominal scale are compared with X2 test and variables measured in numerical scales are compared with t-student test. The p value = <0.05 is used to declare statistically significance difference for all comparisons. Data are entered and analyzed using STATA 10® Data Analysis Statistical Software (Texas, USA).
Results
One hundred eighty six patients are included, the mean age is 28.8 years old (±9.6). One hundred sixty eight (90.3%) patients are male and 18 (9.7%) patients are female. One hundred and nine (59%) patients met criteria for PATI, and 77 (41%) patients are classified as PAT/OT.
The general mean of time from trauma to hospitalization is 90 minutes (±66). The mean of time from trauma to hospitalization in PATI group, is 87 minutes (±53); while in PAT/OT group is 93 minutes (±82), there is not statistically significance difference (p = 0.284).
There are 92 (84%) patients with intoxications (alcohol and/or drugs) in PATI group, and there are 60 (78%) patients with intoxication in PAT/OT group, there is not statistically significance difference (p = 0.26). The organ more affected in both groups is large bowel, followed by small bowel and solid organs. The rest is shown in table 1.
Table 1. Organs injured by number of patients and percentages
|
Organs |
PATI |
% |
PAT/OT |
% |
|
Stomach |
15 |
13.8 |
21 |
27.3 |
|
Duodenum |
3 |
2.7 |
2 |
2.6 |
|
Small bowel |
55 |
50 |
33 |
42.3 |
|
Large bowel |
55 |
50 |
42 |
54.5 |
|
Liver |
19 |
17.4 |
15 |
19.5 |
|
Spleen |
5 |
4.6 |
20 |
26 |
|
Kidney |
2 |
1.8 |
1 |
1.3 |
|
Bladder |
7 |
6.4 |
2 |
2.6 |
|
Pancreas |
0 |
0 |
2 |
2.6 |
|
Diaphragm |
0 |
0 |
22 |
28.6 |
|
Total |
161 |
- |
160 |
- |
|
Source: Electronic files – HGCJ |
||||
Ninety five (87.2%) patients have leukocytosis in PATI group, whereas 67 (87%) patients have leukocytosis in PAT/OT group, there is not statistically significance difference (p = 0.977). The mean of WBC for all patients is 15,100 per mm3 (±4.200); the mean of WBC for PATI group is 14,200 per mm3 (±3.500); whereas, whereas the mean of WBC for PAT/OT group is 16,400 per mm3 (±4.700) (p = 0.01). The mean of hemoglobin level is 13.7 gr/dL (±2.4) in PATI group, the mean of hemoglobin level is 12.8 gr/dL (±2.1) in PAT/OT, there is not statistical significance difference (p = 0.069). The mean of hospital stay for all patients is 9.5 days (±10); the mean of hospital stay for PATI is 8.2 days (±7) and the mean of hospital stay for PAT/OT is 11.6 days (±13), there is statistical significance difference (p = 0.039) (table 2).
Table 2. Comparative of laboratory variables by groups and p value.
|
Laboratory variable |
PATI |
PAT/OT |
Total |
p |
|
Leukocytosis [yes (%)] |
95 (87%) |
67 (87%) |
162 |
0.977 * |
|
WBC mean (per mm3) |
14,200 |
16,400 |
15,100 |
0.01 ** |
|
Hemoglobin mean (gr/dL) |
13.7 |
12.8 |
13.3 |
0.069 ** |
|
Hospital Stay (days) |
8.2 |
11.6 |
9.5 |
0.039 ** |
|
* X2 test ; ** t-Student test Source: Electronic Files - HGCJ |
||||
In PAT/OT group, there are 20 (26%) patients with PAT and thoracic injury (PAT/T) with leukocytosis mean level of 17,400 per mm3 (±5.165); thirteen (17%) patients with PAT and any arm fracture (PAT/A) with leukocytes mean level of 14,100 per mm3 (±3,240); eighteen (23.4%) patients with PAT and any leg fracture (PAT/L) with leukocytosis mean level of 17,100 per mm3 (±3,600); six (8%) patients with PAT and arm also leg fracture (PAT/AL) with leukocytosis mean level of 15.300 per mm3 (±5.500); ten (13%) patients with PAT and thoracic also arms injury (PAT/TA) with leukocytosis mean level of 15.700 per mm3 (±5.800); seven (9%) patients with PAT and thoracic also leg injury (PAT/TL) with leukocytosis mean level of 17.300 per mm3 (±5.200); and 3 (4%) patients with PAT and thoracic also arm and leg injury (PAT/TAL) with leukocytosis mean level of 19.000 per mm3 (±4,6,200). There is not statistical significance difference between these groups and its leukocytosis level (p = 0.594) (figure 1).
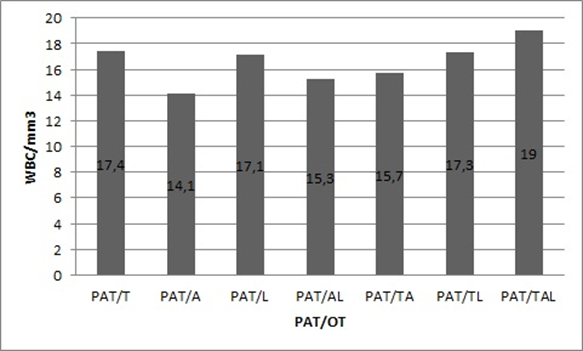
Figure 1. WBC count in patients with PAT/OT separated by regions.
Source: Electronic Files – HGCJ.
Discussion
The purpose of this study is to compare preoperative levels of leukocytosis in patients with PATI and PAT/OT that are underwent to exploratory laparotomy, and observe if the PAT and associated injured in extremities and/or thorax have a major inflammatory response that could mean major leukocytosis.
Diverse Mexican10-13 and international14-16 studies in PAT have shown that productive aged and male gender are the most affected population, this study confirm this statement. The mean of time from injury occurs to hospitalization is 90 minutes, there are not similar studies to compare to this mean, except an anterior study published in patients that were underwent to damage control surgery17. In that study the mean of time from injury to hospitalization was 55 minutes, but context of patients was different.
Prevalence of intoxication does not play an important role in both groups (PATI and PAT/OT). In a previous study, there are not relation between alterations of conscience by drugs and/or alcohol and incidence of non-therapeutic laparotomy18.
Several studies shown that solid organs are the most injured during penetrating trauma, followed by large bowel as the second most injured organ19-21. In this study, large bowel is first in frequency, followed by small bowel and solid organs in third place.
The results shown that both groups have leukocytosis (inflammatory response), but PAT/OT group presents major leukocytosis, with statistically significance difference in favor to this group. Several studies have described a significant higher WBC count (> 12,500 per mm3) in their most severely injured trauma patients3,5,7.
An elevation of WBC count typically reflects the normal response of bone marrow to an infectious or inflammatory process. In case of trauma stimuli, leukocytosis is the appropriate response of bone marrow to these external stimuli6. The metabolic responses to injury and critical illness include hypermetabolism, accelerated skeletal muscle protein breakdown, glucose intolerance, and insulin resistance22. Neutrophils are predominant cells in moderate and severe leukocytosis (called neutrophilia), and are caused by increased of both release from marrow stores and production, plus extended survival and demargination within vessels23.
The integral evaluation of PAT aims to identify patients in need of treatment surgical or non-surgical, and laboratory parameters as a severe leukocytosis may be an early marker for organ or region injured associated with other lesions that may be unsuspected. There is not statistically significance difference in leukocytosis level between the subgroups of PAT/OT. Also, the mean of hemoglobin has not statistically significance difference between groups. The hospital stay is more prolonged in patients with associated trauma, because, these patients suffered any fractures and/or hemothorax, neumothorax and these injuries need specific treatment.
However, despite great advances in the understanding of immune system made in recent decades, little progress has been made regarding the clinical significance of leukocytosis in trauma patients. Results in this study support that higher WBC count is finding in patients with major injuries. A significant elevation in WBC in PAT/OT patients is a phenomenon awaited, and it suggests severe injury and major inflammatory response.
Conflicts of interest: The authors declare that they not have conflicts of interest.
Funding sources: This study not have external funding sources.
Literature cited
1. Centers for Desease Control and Prevention. WISQARS Details of Leading Causes of Death. Atlanta: Office of Statistics and Programming, National Center for Injury Prevention and Control, Centers for Disease Control and Prevention; 2014.
2. Offner PO. Penetrating abdominal trauma. New York: Medscape; 2014.
3. Paladino L, Subramanian R, Bonilla E, Sinert RH. Leukocytosis as prognostic indicator of major injury. West J Emerg Med 2010; 11(5):450-5.
4. Gaona C. Interpretación clínica de la biometría hemática. Med Univer 2003;5(18):35-40.
5. Santucci C, Purcell T, Mejia C. Leukocytosis as a predictor of severe injury in blunt trauma. West J Emerg Med 2008; 9(2):81-5.
6. Abramson N, Melton B. Leukocytosis: basics of clinical assessment. Am Fam Physician 2000; 62(9):2053-60.
7. Díaz-Rosales J, Enríquez-Domínguez L, Castillo-Moreno JR, Herrera-Ramírez F. Preoperative leukocytosis as a predictor of intrabdominal injury in penetrating abdominal trauma. Cir Ciruj 2012; 80(6):516-22.
8. Díaz PP, Olay GF, Hernández RG, Cervantes-Villagrana RD, Presno-Bernal JM, et al. Determinación de los intervalos de referencia de biometría hemática en población mexicana. Rev Latinoamer Patol Clin 2012; 59(4):243-50.
9. Hurtado RM, Mellado YO, Flores GR, Varvas PV. Semiología de la citometría hemática. Rev Fac Med UNAM 2010; 53(4):36-43.
10. Pinedo-Onofre J, Guevara-Torres L, Sánchez-Aguilar J. Penetrating abdominal trauma. Cir Ciruj 2006; 74(6):431-42.
11. Senado-Lara I, Castro-Mendoza A, Palacio-Vélez F, Vargas-Avila A. Experience in management of trauma-related acute abdomen at the “General Ignacio Zaragoza” Regional Hospital in Mexico City. Cir Ciruj 2004; 72(2):93-7.
12. Sánchez Lozada R, González Ortiz J, Soto Villagrán R. Lesiones abdominales por trauma: experiencia de dos años en un hospital de tercer nivel. Cir Gen 2002; 24(3):201-5.
13. Rodríguez-Paz C, González de Blas J, Carreón-Bringas R. Manejo de trauma abdominal en dos hospitales rurales de San Luis Potosí. Trauma 2008; 11(1):21-4.
14. Zafar S, Rushing A, Haut E, Kisat M, Villegas C, Chi A, et al. Outcome of selective non-operative management of penetrating abdominal injuries from the North American National Trauma Database. Br J Surg 2012; 99 (Suppl 1):155-64.
15. Navsaria P, Berli J, Edu S, Nicol A. Non-operative management of abdominal stab wounds--an analysis of 186 patients. S Afr J Surg 2007; 45(4):128-30.
16. Bocic G, Poblete J, Munita J, Korn O, Guiñez R, Urrutia L, et al. Heridas cortopunzantes penetrantes abdominales. Rev Chil Cir 1994; 46(4):404-9.
17. Enríquez-Domínguez L, Díaz-Rosales J, Herrera-Ramírez F, Castillo-Moreno J. Cirugía de control de daño. Experiencia inicial en el Hospital General de Ciudad Juárez, México, durante el periodo de abril del 2008 a diciembre del 2010. Med UIS 2011; 24(2):195-9.
18. Castillo-Moreno JR, Enríquez-Domínguez L, Herrera-Ramírez F, Díaz-Rosales J. Laparotomía no-terapéutica en trauma penetrante abdominal y su relación con el estado de intoxicación por alcohol y drogas. Cir Gen 2011; 33:232-5.
19. Pedroza J, Delgadillo S. Trauma de colon manejado con colostomía. An Med (Mex) 2011; 56(1):20-4.
20. Tapia A, Raddatz A, Zuñiga J, Venezian E, Larraín E, Saa E. Hallazgos quirúrgicos en pacientes con shock por heridas penetrantes abdominales por arma blanca. Rev Chi Cir 1994; 46(4):410-13.
21. Raddatz A. Tapia A, Larrain E, Saa E, Venezian E, Zúñiga J, et al. Heridas penetrantes abdominales por arma blanca: análisis de 500 pacientes operados. Rev Chi Cir 1992; 42(2):215-21.
22. Bessey P, Lowe K. Early hormonal changes affect the catabolic response to trauma. Ann Surg 1993; 218(4):476-91.
23. Lawrence Y, Raveh D, Rudensky B, Munter G. Extreme leukocytosis in the emergency department. Q J Med 2007; 100(4):217-23.
![]()