Minilaparotomy approach for biliary ileus: Case report
Juan de Dios Díaz-Rosales, MD, MSc.1*, Lenin Enríquez-Domínguez, MD.2*
1* General Surgeon, Surgery Service/Hospital General Regional No. 66 - IMSS. Sciences Health Department / Universidad Autónoma de Ciudad Juárez. México. Correo: jdedios.uacj@gmail.com
2* General Surgeon, Surgery Service/Hospital General Regional No. 66 - IMSS. Sciences Health Department / Universidad Autónoma de Ciudad Juárez. México. Correo: lenin_enriquez@hotmail.com
Archivos de Medicina (Manizales), Volumen 15 N° 2, Julio-Diciembre 2015, ISSN versión impresa 1657-320X, ISSN versión en línea 2339-3874. Díaz Rosales, J.D.; Enríquez-Domínguez L.
Recibido para publicación: 05-05-2015 - Versión corregida: 21-09-2015 - Aprobado para publicación: 10-11-2015
Summary
Introduction: Biliary ileus is a rare cause of mechanical bowel obstruction and results from the passage of gallstones into the small bowel. Case presentation: A 62-year old woman with episode of biliary ileus is underwent to minilaparotomy (5 cm) to extract gallstone from small bowel. Posteriorly, the patient was discharged on postoperative day 5 without any complication. Conclusion: Minilaparotomy approach is a safe and feasible option in patients with highly suspected diagnosis in centers without laparoscopy devices or surgery, with excellent results when one-stage procedure is not considered.
Keywords: gallstones, cholelithiasis, intestinal obstruction, laparotomy, general surgery.
Díaz-Rosales JD, Enríquez-Domínguez L. Minilaparotomy approach for biliary ileus: case report. Arch Med (Manizales) 2015; 15(2):352-6.
Abordaje por minilaparotomía para íleo biliar: Reporte de caso
Resumen
Introducción: El íleo biliar es una causa mecánica poco frecuente de obstrucción intestinal y es resultado del paso de un lito biliar hacia la luz intestinal. Presentación del caso: Paciente femenino de 62 años con diagnóstico de íleo biliar es sometida a una minilaparotomía (incisión de 5 cms) para extraer el lito del lumen intestinal. La paciente es dada de alta el día 5 del postoperatorio sin complicaciones. Conclusión: En centros donde no se cuanta con equipo o cirugía laparoscópica, el abordaje por minilaparotomía es una opción factible, segura y con excelentes resultados en pacientes con alta sospecha diagnóstica.
Palabras clave: cálculos biliares, colelitiasis, obstrucción intestinal, laparotomía, cirugía general.
Introduction
Biliary ileus is a rare etiology of mechanical bowel obstruction, due to the existence of a fistula between the biliary tree and the digestive tract1. Most patients are over age 65, and have associated several medical conditions, which contribute to a high morbidity and mortality rates2, therefore this condition requires emergency treatment. There are different options in approach, however, open vs laparoscopic are the main options3-5. The objective of this article is reports the use of minilaparotomy without biliary tract surgery in the approach of biliary ileus.
Case presentation
A 62-year-old woman with complaints of abdominal pain, nausea and bilious vomits of 1 week evolution is evaluated in emergency room (ER). She has history of hypertension and type 2 diabetes with no other significant medical or surgical history. On general examination, the patient is moderately dehydrated with acute renal failure (urea 146.5 mg/dL, BUN 68.5 mg/dL, creatinine 3.9 mg/dL) and hemodynamically stable (BP 100/70 mmHg, 65 BPM). Abdominal examination reveals moderate abdominal distention without palpable masses or hernias. Signs of peritoneal irritation are absent, but nasogastric tube reveals fecaloid liquid.
Biometry hematic shows hemoglobin 17.4 gr/dL, hematocrit 47.9%, WBC 9900/mm3, neutrophils 69%. Liver function test shows total bilirubin 0.69 mg/dL, direct bilirubin 0.09 mg/dL, indirect bilirubin 0.6 mg/dL, ALT 18 UI/L, AST 23 UI/L, GGT 74 UI/L, and, alkaline phosphatase 91 UI/L.
Abdominal radiography reveals distended loops of small bowel, and a round calcified body in the right lower quadrant (figure 1). The abdominal ultrasonography shows suggestive data of cholelithiasis and cholecystitis. A suspicious diagnosis of biliary ileus is made, and emergency minilaparotomy is performed. Transumbilical incision of 5 cm is performed, enough to take the distal ileum, and explore it. Into lumen of distal ileum an impacted gallstone is found (figure 2). Longitudinal enterolithotomy is performed to extract the stone (measures 33 mm x 24 mm) (figure 3), the intestinal incision is closed transversely using Lembert suture. Abdominal wall is closed with routinary technique (in mass).
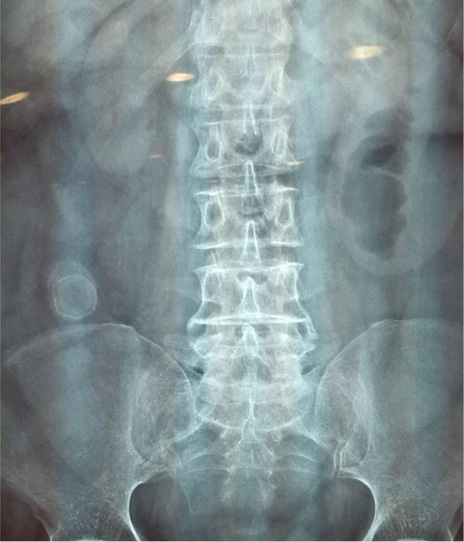
Figure 1. Abdominal x ray reveals a calcified round body in right lower quadrant (source: clinic file).


Figure 2. (A) Gallstone is found at distal ileum, (B) longitudinal enterolithotomy is performed to extract the stone (source: clinic file).

Figure 3. Pigmented and calcified gallstone (source: clinic file).
The patient resumed oral intake on postoperative day 2 and is discharged on postoperative day 5. The patient is followed in surgical consult for any complication at week 1, 3, and 6.
Because endoscopy service is not a routinary auxiliary tool, the endoscopic retrograde cholangiopancreatography is not performed, but 1-year follow up, the patient is without biliary complications.
Discussion
Although some medical centers make right diagnosis using advanced imaging (CT allows direct visualization of cholecystoenteric fistula)6, in centers without this technology, the diagnosis is based on clinical suspicious (Rigler triad: air-fluid levels, aerobilia and radiopaque gallstone in atypical position)7. Little more aggressive than laparoscopy and less invasive than traditional laparotomy, minilaparotomy is a valid therapeutic approach and is recommended when diagnosis of biliary ileus is high suspected.
There are discussion about one-stage procedure (enterolithotomy, cholecystectomy and fistula repair) versus enterolithotomy alone8-11. But, some authors suggest the second option, because spontaneous closure of a fistula can occur within a month of onset of biliary ileus8 and complications such as recurrent biliary ileus and chronic cholangitis even cancer, occurs rarely9,10.
It is considered that one-stage procedure is unnecessary in majority cases, because it is associated with a prolonged surgical time, higher complications mortality rates than enterolithotomy alone procedure. For those surgeons that biliary surgery is a mandatory option, it is recommended delayed elective cholecystectomy and fistula repair during the quiet period 3-6 months after biliary ileus surgery11.
Conclusion
Minilaparotomy approach is a feasible option in centers without laparoscopy surgery or in patients with contraindications for laparoscopic procedures, with excellent results when one-stage procedure is not considered.
Conflict of interest statement: The authors have no conflict of interests to declare.
Funding sources: None
Literature cited
1. Echenique EM, Amondaraín AJA, Lirón de Robles SC. Biliary ileus. Rev Esp Enferm Dig 2007; 99(11):672-680
2. Clavien PA, Richon J, Burgan S, Rohne A. Gallstone ileus. Br J Surg 1990; 77(7):737-742
3. Ruvikumar R, Williams JG. The operative management of gallstone ileus. Ann R Coll Surg Engl 2010; 92:279-281
4. Gupta RA, Shah CR, Balsara KP. Laparoscopic-assisted enterolithotomy for gallstone ileus. Indian J Surg 2013; 75(Suppl 1):S497-S499
5. Paiva-Coronel G, Martínez-Ramos D, Cosa-Rodríguez R, Salvador-Sanchis JL. Biliary ileum. Assisted laparoscopic approach. Cir Esp 2010; 87(4):252-264
6. Michele D, Luciano G, Massimiliano F, Stefano R, Roberta D, Ernesto S, et al. Usufulness of CT-scan in the diagnosis and therapeutic approach of gallstone ileus: report of two surgically treated cases. BMC Surgery 2013; 13(Suppl 2):S6
7. Roothans D, Anguille S. Rigler triad in gallstone ileus. CMAJ 2013; 185(14):E690.
8. Shioi Y, Kawamura S, KAnno K, Nishuinari Y, Ikeda K, Noro A, et al. A case of gallstone ileus displaying spontaneous closure of cholecystoduodenal fistula after enterolithotomy. Int J Surg Case Rep 2012; 3(1):12-15
9. Jones R, Broman D, Hawkins R, Coless D. Twice recurrent gallstone ileus: a case report. J Med Case Reports 2012; 6:362
10. Hayes N, Saha S. Recurrent gallstone ileus. Clin Med Res 2012; 10(4):236-239
11. Ayantunde AA, Agrawal A. Gallstone ileus: diagnosis and management. World J Surg 2007; 31(6):1294-1299
