Jaime Andrés Pardo Romero1 , Cristian Hincapié Porras2, Leidy Alexandra Guzmán Polanía3, Natalia Andrea Torres Valencia4
Recibido para publicación: 26-11-2025. Versión corregida: 29-04-2026. Aprobado para publicación: 03-06-2025.
Modelo de citación:
Pardo Romero J.A., Hincapié Porras C., Guzmán Polanía L.A., Torres Valencia N.A. Cardioversión farmacológica transplacentaria con digoxina en un feto hidrópico: informe de un caso. Arch Med (Manizales). 2026;26(1). https://doi.org/10.30554/archmed.26.1.5567.2026
Introduction: Fetal arrhythmias are conditions that occur in a small percentage of pregnancies, diagnosed incidentally via ultrasound. Most arrhythmias are fetal tach- yarrhythmias, which can complicate the course of pregnancy, causing fetal heart failure and fetal hydrops in untreated cases and increasing rates of perinatal morbidity and mortality. Case presentation: This is a 38-year-old patient, 27.6 weeks pregnant, who was admitted to a tertiary care facility following the detection of foetal tachycardia during an obstetric ultrasound scan. The foetal echocardiogram confirmed a tachyarrhythmia of the supraventricular tachycardia type and foetal hydrops, the latter finding due to the presence of ascites and pericardial effusion. Fetal structural anatomical pathology was ruled out; laboratory tests performed on the patient ruled out Rh incompatibility, thyroid disease and TORCH complex infections (toxoplasmosis, rubella, cytomegalovirus, herpes, syphilis, hepatitis B and HIV). Subsequently, transplacental pharmacological cardioversion with digoxin was performed, achieving a return to sinus rhythm and resolution of the hydrops after three weeks of treatment. This allowed the pregnancy to be carried to term at 37.0 weeks without any complications. Conclusion: Although the incidence of foetal arrhythmias is low, timely and e y diagnosis and treatment in institutions with trained staff can reduce perinatal complications and enable full-term pregnancies. Furthermore, the efficacy of digoxin as an antiarrhythmic agent was
![]()
Universidad Libre, Calí, Valle del Cauca, Colombia.
ORCID: https://orcid.org/0009-0006-1339-2818. Correo: jaimea-pardor@unilibre.edu.co.
Korial Group, Medicina Materno Fetal Integral, Pereira, Risaralda, Colombia. ORCID: https://orcid.org/0000-0001-5816-6511. Correo: cristianhincapie@gmail.com.
Korial Group, Medicina Materno Fetal Integral, Pereira, Risaralda, Colombia. ORCID: https://orcid.org/0009-0003-6244-3392. Correo: leidy.guzman@gmail.com.
Korial Group, Medicina Materno Fetal Integral, Pereira, Risaralda, Colombia. ORCID: https://orcid.org/0000-0001-9345-2847. Correo: natorres@fucsalud.edu.co.
Pardo Romero J.A., Hincapié Porras C., Guzmán Polanía L.A., Torres Valencia N.A. Cardioversión farmacológica transplacentaria con digoxina en un feto hidrópico: informe de un caso.
Arch Med (Manizales). 2026;26(1)
demonstrated, even in hydropic foetuses where the return to sinus rhythm may take longer than usual compared to foetuses without foetal hydrops.
Keywords: Fetal arrhythmias, fetal supraventricular tachycardia, fetal hydrops.
Introducción: Las arritmias fetales son afecciones que se producen en un pequeño porcentaje de embarazos y que se diagnostican de forma incidental mediante eco- grafía. La mayoría de las arritmias son taquiarritmias fetales, que pueden complicar el curso del embarazo, provocando insuficiencia cardíaca fetal e hidropesía fetal en los casos no tratados, y aumentando las tasas de morbilidad y mortalidad perinatal. Presentación del caso: Presentamos el caso de una paciente de 38 años, con 27,6 semanas de gestación, que ingresó en un centro de atención terciaria tras la detección de taquicardia fetal en una ecografía obstétrica. La ecocardiografía fetal confirmó una taquiarritmia supraventricular e hidropesía fetal, este último hallazgo evidenciado por la presencia de ascitis y derrame pericárdico. Se descartó una patología anatómica estructural fetal, y las pruebas paraclínicas realizadas a la paciente descartaron incom- patibilidad Rh, patología tiroidea e infecciones del complejo TORCH (toxoplasmosis, rubéola, citomegalovirus, herpes, sífilis, hepatitis B y VIH). Posteriormente, se realizó una cardioversión farmacológica transplacentaria con digoxina, logrando el retorno al ritmo sinusal y la resolución del hidropesía tras tres semanas de tratamiento. Esto permitió llevar el embarazo a término a las 37 semanas sin complicaciones. Conclu- sión: Aunque la incidencia de arritmias fetales es baja, el diagnóstico y el tratamiento oportunos en centros con personal capacitado reducen las complicaciones perinata- les y permiten llevar los embarazos a término. Además, se demostró la eficacia de la digoxina como agente antiarrítmico, incluso en fetos con hidropesía, en los que el retorno al ritmo sinusal puede tardar más de lo habitual en comparación con los fetos sin hidropesía fetal.
Palabras clave: Arritmias fetales, taquicardia supraventricular fetal, hidropesía fetal.
Introdução: As arritmias fetais são condições que ocorrem numa pequena percentagem de gravidezes e que são diagnosticadas de forma incidental através da ecografia. A maioria das arritmias são taquiarritmias fetais, que podem complicar o curso da gravi- dez, provocando insuficiência cardíaca fetal e hidropisia fetal nos casos não tratados,
Pardo Romero J.A., Hincapié Porras C., Guzmán Polanía L.A., Torres Valencia N.A. Cardioversión farmacológica transplacentaria con digoxina en un feto hidrópico: informe de un caso.
Arch Med (Manizales). 2026;26(1)
e aumentando as taxas de morbidade e mortalidade perinatal. Apresentação do caso: Apresentamos o caso de uma paciente de 38 anos, com 27,6 semanas de gestação, que deu entrada num centro de cuidados terciários após a deteção de taquicardia fetal numa ecografia obstétrica. A ecocardiografia fetal confirmou uma taquiarritmia supra- ventricular e hidropisia fetal, este último achado evidenciado pela presença de ascite e derrame pericárdico. Foi descartada uma patologia anatómica estrutural fetal, e os exames paraclínicos realizados à paciente descartaram incompatibilidade Rh, patologia tireoidiana e infeções do complexo TORCH (toxoplasmose, rubéola, citomegalovírus, herpes, sífilis, hepatite B e VIH). Posteriormente, foi realizada uma cardioversão far- macológica transplacentária com digoxina, conseguindo-se o retorno ao ritmo sinusal e a resolução da hidropisia após três semanas de tratamento. Isto permitiu levar a gravidez a termo às 37 semanas sem complicações. Conclusão: Embora a incidência de arritmias fetais seja baixa, o diagnóstico e o tratamento oportunos em centros com pessoal qualificado reduzem as complicações perinatais e permitem levar as gravidezes a termo. Além disso, foi demonstrada a eficácia da digoxina como agente antiarrítmico, mesmo em fetos com hidropisia, nos quais o retorno ao ritmo sinusal pode demorar mais do que o habitual em comparação com fetos sem hidropisia fetal.
Palavras-chave: Arritmias fetais, taquicardia supraventricular fetal, hidropisia fetal.
Fetal arrhythmias are defined as an alteration in the rhythm of the cardiac cycle [1] diagnosed by ultrasound; they complicate up to 1% of pregnancies, the majority of which are due to benign conditions; however, tachyarrhythmias can cause haemodynamic decompensation, hydrops and foetal death [2]. Early detection in preterm pregnancies allows for the use of various antiarrhythmic drugs, which help pre- vent haemodynamic changes and restore sinus rhythm; however, in foetuses with hydrops, there may be no response or it may take a longer period of time to restore sinus rhythm.
We present the case of a 38-year-old patient from a rural area, a housewife, with an obstetric history of G2C1V1, blood group A positive, at
27.6 weeks’ gestation according to a late-stage ultrasound scan, with no significant medical history. The patient was admitted to the A&E department of a tertiary care hospital, asymp- tomatic, following findings of foetal tachycardia on an obstetric ultrasound scan. On admission
to the obstetrics ward, foetal tachycardia (232 beats per minute) was confirmed by Doppler, with vital signs: blood pressure 114/78 mmHg, heart rate 72 beats per minute, respiratory rate 16 breaths per minute, oxygen saturation 98% (FiO2 21%), temperature 36.1°C.
Physical examination: fundal height 25 centimetres, no uterine activity, no uterine tenderness, foetal movements present, no am- niorrhea, no genital bleeding and a body mass index of 23.1.
A foetal echocardiogram was performed, revealing no structural anatomical abnormali- ties, but showing supraventricular tachycardia with an atrioventricular ratio of 1:1 and a heart rate of 240 beats per minute (Figure 1), and foetal hydrops due to the presence of ascites and pericardial effusion (Figure 2); in addition, hydrocele and polyhydramnios. Admission lab- oratory results showed the following blood pa- rameters: white blood cells 7,800 μL, C-reactive protein (CRP) at 0.3 mg/L, urine analysis and
Pardo Romero J.A., Hincapié Porras C., Guzmán Polanía L.A., Torres Valencia N.A. Cardioversión farmacológica transplacentaria con digoxina en un feto hidrópico: informe de un caso.
Arch Med (Manizales). 2026;26(1)
urine Gram stain non-pathological, thyroid-stim- ulating hormone (TSH) at 2.7 mIU/L and free thyroxine (T4L) 1.1 ng/dl. TORCH complex infections (toxoplasmosis, rubella, cytomega- lovirus, herpes, syphilis, hepatitis B and HIV) were ruled out to exclude other aetiologies of foetal hydrops.
Prior to the start of antiarrhythmic treatment, the patient underwent renal function tests, elec- trolyte tests, a transthoracic echocardiogram and a cardiology assessment; in the absence of contraindications and with diagnostic pa- rameters within normal limits, pharmacological treatment with digoxin was initiated.
The patient was transferred to the obstetric intensive care unit; treatment was initiated with
betamethasone to induce foetal maturation, and transplacental drug therapy with intravenous digoxin was started (loading dose of 0.5 mg every 8 hours for 4 days), under continuous maternal and foetal monitoring, due to the risk of digoxin toxicity. On day four, serum digoxin levels were measured and found to be within the therapeutic range (1.3 ng/ml), and the patient was subsequently switched to oral digoxin 0.25 mg/ e every 12 hours. She was subsequently transferred to the gynaecology and obstetrics ward, and a return to foetal sinus rhythm (Fig- ure 3) was achieved within two weeks, with res- olution of the hydrops four weeks after treatment began. She was discharged on oral digoxin at a dose of 0.25 mg orally every 12 hours and weekly follow-up in the outpatient clinic of the maternal-foetal medicine department until the end of the pregnancy at 37 weeks.
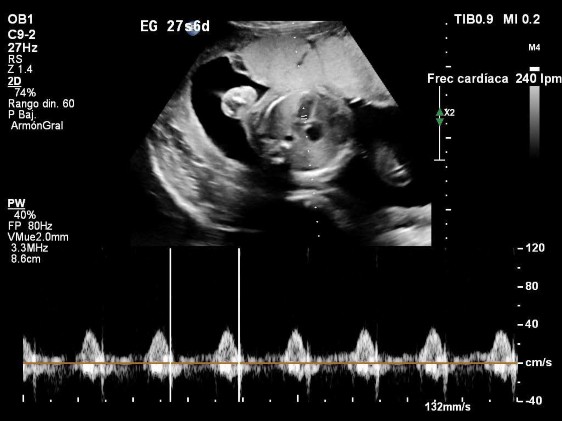
Figure 1. Transabdominal obstetric ultrasound, 27.6-week pregnancy showing evidence of foetal tachycardia with a heart rate of 240 beats per minute. Four-chamber view.
Pardo Romero J.A., Hincapié Porras C., Guzmán Polanía L.A., Torres Valencia N.A. Cardioversión farmacológica transplacentaria con digoxina en un feto hidrópico: informe de un caso.
Arch Med (Manizales). 2026;26(1)

Figure 2. Transabdominal obstetric ultrasound, 27.6 weeks’ gestation. In the image on the left, showing a cross-section of the foetal abdomen, ascites is observed; in the image on the right, pericardial effusion is observed in the four-chamber view, findings consistent with foetal hydrops.
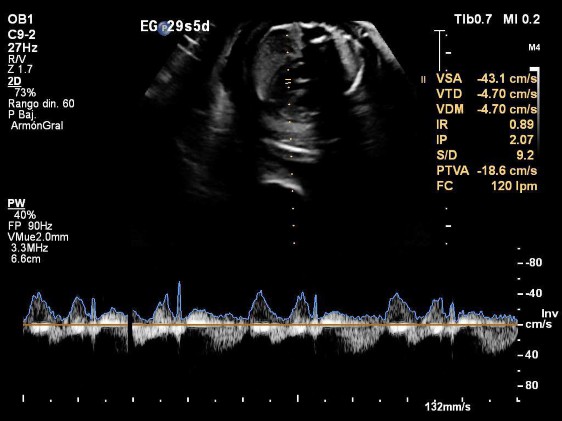
Figure 3. Transabdominal obstetric ultrasound, 29.5 weeks’ gestation, showing a foetus with a normal foetal heart rate in the four-chamber view, following initiation of digoxin therapy.
Pardo Romero J.A., Hincapié Porras C., Guzmán Polanía L.A., Torres Valencia N.A. Cardioversión farmacológica transplacentaria con digoxina en un feto hidrópico: informe de un caso.
Arch Med (Manizales). 2026;26(1)
Follow-up and results Discussion
During outpatient clinical and ultrasound fol- low-up by the maternal-foetal medicine depart- ment, the foetus remained in sinus rhythm, with normal foetal heart rates and no recurrence of foetal hydrops (Figure 4). The patient showed no intolerance or signs of digoxin toxicity. The pregnancy was terminated at 37.0 weeks by caesarean section due to a history of previous caesarean section. There were no complica- tions during the caesarean section; a newborn was delivered with a normal heart rate, weighing over 2,500 grams, with adequate neonatal ad- aptation, no major malformations, and a normal postnatal echocardiogram.
This case involves a pregnant woman in whom foetal tachycardia was detected at 27.6 weeks, who subsequently developed foetal hydrops. The complexity of the case lies in the management of multiple conditions that posed a risk to both foetal and maternal well-being.
Fetal arrhythmias are defined as an irregu- lar heart rhythm [1], with an abnormally low or high heart rate, known as fetal bradycardia or fetal tachycardia, respectively; however, the incidence of fetal arrhythmias is less than 2% of all pregnancies [2]. Most are diagnosed using ultrasound (obstetric ultrasound, Doppler) and foetal echocardiography. The latter is a funda- mental tool for the prenatal assessment of the foetal heart, as it allows the majority of foetal arrhythmias to be distinguished with significant diagnostic accuracy [3].
With regard to foetal tachycardias, the most common are sinus tachycardia, atrial fibrillation, ventricular tachycardia and su- praventricular tachycardia [4]; all typically have heart rates exceeding 200 beats per minute. Despite their low incidence, some of these arrhythmias are associated with high morbidity and mortality [5]; some may go
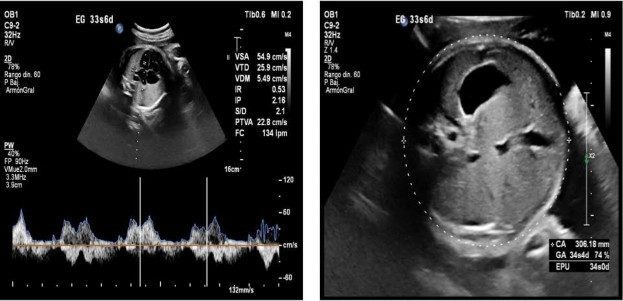
Figure 4. Transabdominal obstetric ultrasound, 33.6 weeks’ gestation. The left-hand image shows a normal foetal heart rate (134 beats per minute) and resolution of the pericardial effusion in the four-chamber view; the right-hand image shows resolution of the ascites in a transverse view of the foetal abdomen.
Pardo Romero J.A., Hincapié Porras C., Guzmán Polanía L.A., Torres Valencia N.A. Cardioversión farmacológica transplacentaria con digoxina en un feto hidrópico: informe de un caso.
Arch Med (Manizales). 2026;26(1)
undiagnosed and lead to up to 10% of foetal deaths, preterm birth [6] and foetal hydrops secondary to heart failure [7].
Furthermore, foetal hydrops is defined as the excessive and pathological accumulation of fluid in two or more body cavities, including the peritoneal cavity, pleural space, pericardium and skin. Although placentomegaly and poly- hydramnios tend to coexist, they are not part of the diagnostic criteria for this condition [8].
The progression of foetal hydrops is usually rapid and progressive when it occurs at earlier gestational ages and in foetuses with higher heart rates.
With regard to foetal tachycardias, foetal supraventricular tachycardia accounts for more than two-thirds of foetal tachycardias, usually presenting at the end of the second trimester and the start of the third trimester [6]. It typically presents with heart rates between 220 and 320 beats per minute. The average time to return to sinus rhythm or cardioversion is approximately 6–7 days after the start of antiarrhythmic treat- ment [9]; however, in cases of foetal hydrops, the rate of cardioversion is slower [10].
With regard to pharmacological therapy, it is indicated for foetuses with elevated heart rates persisting for more than 12 hours and a gesta- tional age of less than 36 weeks; these should receive transplacental pharmacological therapy. Currently, three first-line drugs are used in the treatment of foetal supraventricular tachycardia: digoxin, flecainide and sotalol [11].
Historically, flecainide and sotalol have shown greater efficacy than digoxin; however, recent evidence suggests that flecainide and digoxin have higher rates of return to sinus rhythm compared to sotalol [10], so the use of digoxin should be considered the first option in settings where other antiarrhythmics are not available, given its proven effectiveness.
Transplacental dosing does not always achieve adequate foetal concentrations; for this reason, the mother may require higher maternal
doses or a combination of multiple antiarrhyth- mic drugs to control the foetal heart rate.
In cases of foetal tachycardia and gestational ages over 36 weeks, the pregnancy may be terminated. However, in recent years, some major centres have recommended the initiation of transplacental therapy to allow for control of the foetal heart rate and to minimise the risk associated with late preterm birth. Another scenario in which transplacental therapy is recommended at gestational ages > 36 weeks is in the case of hydropic foetuses, as it may improve pulmonary function [9].
When assessing a pregnant woman with foe- tal arrhythmia, one of the first diagnostic tests to be performed is a foetal echocardiogram to determine the type of foetal arrhythmia and rule out any structural abnormalities. Once the type of arrhythmia has been determined, the appropriate antiarrhythmic drug can be select- ed. Fetal supraventricular tachycardia presents a significant challenge in obstetric practice, as it is a condition requiring timely diagnosis and treatment, given its major implications for the normal course of pregnancy, such as foetal death, preterm birth and heart failure leading to foetal hydrops. The presence of foetal hy- drops as a complication significantly increases morbidity and mortality, with mortality rates reaching up to 27% in untreated cases. In cases of associated foetal hydrops, the time taken to convert to sinus rhythm is usually longer and, in some cases, conversion is unsuccessful. Transplacental pharmacological management is the cornerstone of treatment. Drugs such as flecainide and sotalol have historically been the first-line options in hydropic foetuses. However, recent evidence suggests that digoxin is as effective as flecainide and more effective than sotalol in restoring foetal sinus rhythm, which is why digoxin could be considered the first-line therapeutic option in situations where other an- tiarrhythmics are not available, as in the present
Pardo Romero J.A., Hincapié Porras C., Guzmán Polanía L.A., Torres Valencia N.A. Cardioversión farmacológica transplacentaria con digoxina en un feto hidrópico: informe de un caso.
Arch Med (Manizales). 2026;26(1)
case. It is advisable to initiate antiarrhythmic C.H.P., L.G. and N.A.T. participated in the therapy early to prevent progression to heart analysis and interpretation of ultrasound data failure, foetal hydrops and foetal death. results, image acquisition, clinical management
of the case, follow-up, manuscript review, and final approval.
The authors state that they obtained written informed consent from the patient for the pub-
lication of photographs and the corresponding The authors declare no conflicts of interest. clinical material. Use of AI
Authors’ contributions The authors declare that artificial intelligence
J.A.P.R. performed clinical data acquisition, was not used in this work. follow-up, and manuscript drafting.
Carvalho JS. Fetal dysrhythmias. Vol. 58, Best Practice and Research: Clinical Obstetrics and Gynaecology. Bailliere Tindall Ltd; 2019. p. 28–41. https://doi.org/10.1016/j.bpobgyn.2019.01.002
Gozar L, Gabor-miklosi D, Toganel R, Fagarasan A, Gozar H, Toma D, et al. Fetal Tachyarrhythmia Management from Digoxin to Amiodarone—A Review. Vol. 11, J Clin Medicine. https://doi.org/10.3390/jcm11030804
Weber R, Stambach D, Jaeggi E. Diagnosis and management of common foetal arrhythmias. Journal of the Saudi Heart Association, editor. Vol. 23. 2011. p. 61–6. https://doi.org/10.1016/j.jsha.2011.01.008
Vedel C, Vejlstrup N, Jensen LN, Ekelund CK, Nørgaard LN, Harmsen L, et al. Refractory Fetal Supraventricular Tachycardia with Hydrops Successfully Converted by Intraperitoneal Flecainide in the Fetus: A Case Report. Fetal Diagn Ther. 1 September 2020;47(9):717–20. https://doi.org/10.1159/000508811
Holmes S, Hornberger LK, Jaeggi E, Howley L, Moon-Grady AJ, Uzun O, et al. Treatment, not delivery, of the late preterm and term foetus with supraventricular arrhythmia. Ultrasound Obstetrics and Gynaecology. 1 October 2023;62(4):552–7. https://doi.org/10.1002/uog.26239
Wacker-Gussmann A, Strasburger JF, Cuneo BF, Wakai RT. Diagnosis and treatment of foetal arrhythmia. Vol. 31, Am J Perinatol. Thieme Medical Publishers, Inc.; 2014. p. 617–28. https://doi.org/10.1055/s-0034-1372430
Swearingen C, Colvin ZA, Leuthner SR. Nonimmune Hydrops Fetalis. Vol. 47, Clinics in Perinatology. W.B. Saun- ders; 2020. p. 105–21. https://doi.org/10.1016/j.clp.2019.10.001
Younge T, Ottolini K, Al-Kouatly H, Berger S. Hydrops fetalis: Incidence, Etiologies, Management Strategies, and Outcomes. Res Rep Neonatol. 20 Dec 2023;Vol. 13:81–92. https://doi.org/10.2147/RRN.S411736
Strasburger JF, Eckstein G, Butler M, Noffke P, Wacker-Gussmann A. Fetal Arrhythmia Diagnosis and Pharma- cologic Management. J Clin Pharmacol. 1 September 2022;62:S53–66. https://doi.org/10.1002/jcph.2129
Jaeggi ET, Carvalho JS, De Groot E, Api O, Clur SAB, Rammeloo L, et al. Comparison of transplacental treatment of foetal supraventricular tachyarrhythmias with digoxin, flecainide, and sotalol: Results of a non-randomised multicentre study. Pediatr Cardiol. 28 October 2011;124(16):1747–54. https://doi.org/10.1161/CIRCULATIONAHA.111.026120
Celentano L, Yoshinaga K, Shiba SK, Gaynor Z, Rudolph J. A Rare and Challenging Case of Refractory Fetal Supraventricular Tachycardia. Cureus. 8 September 2022;14(9):e28947.
https://doi.org/10.7759/cureus.28947
![]()