Jorge Oliveros-Rivero1 , Gabriela Fajardo-Ponce2
Received for publication: 28 June 2025. Revised version: 15 November 2025. Approved for publication: 16 April 2026.
Modelo de citación:
Oliveros-Rivero J., Fajardo-Ponce G. Congenital rectal atresia: a rare malformation that may go unnoticed. Case report. Arch Med (Manizales). 2026;26(1). https://doi.org/10.30554/archmed.26.1.5433.2026
![]()
Paediatric Surgeon. Paediatric Surgery Department. Monte Sinaí General Hospital. Guayaquil, Ecuador. ORCID: https://orcid.org/0000-0002-0824-0864. Email: jorgealejandrooliveros@hotmail.com.
Paediatric Surgeon. Paediatric Surgery Department. Monte Sinaí General Hospital. Guayaquil, Ecuador. ORCID: https://orcid.org/0000-0003-3698-0867. Email: gabrielita_fp@hotmail.com.
Oliveros-Rivero J., Fajardo-Ponce G.
Congenital rectal atresia: a rare malformation that may go unnoticed. Case report.
Arch Med (Manizales). 2026;26(1)
Atresia rectal congénita: una malformación rara que puede pasar desapercibida
Oliveros-Rivero J., Fajardo-Ponce G.
Congenital rectal atresia: a rare malformation that may go unnoticed. Case report.
Arch Med (Manizales). 2026;26(1)
o diagnóstico. O exame físico neonatal deve incluir a verificação instrumental da permeabilidade anal. A abordagem cirúrgica escalonada permitiu a estabilização do paciente, o diagnóstico definitivo e a reconstrução bem-sucedida, em concordância com o relatado na literatura. Conclusão: Deve-se suspeitar de atresia retal em recém-
-nascidos com sinais de obstrução intestinal baixa, apesar de um ânus de aparência normal. O diagnóstico precoce e o tratamento cirúrgico oportuno são fundamentais para um desfecho favorável.
congenital rectal atresia is a rare anorectal malformation, accounting for between 0.3% and 2% of such defects [1,2]. It is characterised by a normal-appearing anus and an interruption of the rectal canal a few centimetres from the dentate line [2]. This anatomical appearance can delay diagnosis if a thorough perineal ex- amination is not performed, thereby increasing the risk of complications such as intestinal perforation [1,3,4].
The clinical presentation includes abdom- inal distension, vomiting and failure to pass meconium, symptoms common to other causes of lower intestinal obstruction [3,4]. The diagnosis is confirmed by digital rectal examination, radiological investigations and contrast studies. Although numerous classifi- cations have been proposed, there is still no standardised system [2].
Surgical treatment is tailored to the individ- ual and includes techniques such as posterior sagittal rectoanal anastomosis, transanal or combined approaches, with good functional outcomes, although constipation is common during follow-up [5–7].
This report describes a case of congenital rectal atresia with a delayed diagnosis, high- lighting the importance of neonatal clinical assessment and a staged surgical approach.
a male newborn, the sole product of a 39-week pregnancy delivered by caesarean section, with an Apgar score of 8-9-9, weigh- ing 3180 g and with no relevant maternal or perinatal history. At , the initial physical assess- ment reported a “permeable anus”; however, he did not pass meconium within the first 24 hours of life.
At 30 hours of life, he developed vomiting with streaks of blood, progressive abdominal distension and chocolate-coloured gastric out- put via an orogastric tube, leading to a suspicion of necrotising enterocolitis and the initiation of medical treatment.
In view of the progressive clinical deterio- ration, with increased gastric output, enlarge- ment of the abdominal circumference and radiological findings of dilated intestinal loops with oedema and air-fluid levels (Figure 1), a diagnosis of intestinal obstruction was con- sidered and he underwent surgery at 3 days of life. During exploratory laparotomy, a 5 cm colonic perforation was identified in the middle portion of the transverse colon, involving more than 80% of its circumference, with leakage of intestinal contents. A colo-colonic anastomosis was performed using 4-0 Vicryl sutures, and a Penrose drain was placed. The cause of the distal obstruction was not identified during this procedure.
Oliveros-Rivero J., Fajardo-Ponce G.
Congenital rectal atresia: a rare malformation that may go unnoticed. Case report.
Arch Med (Manizales). 2026;26(1)

Figure 1. Preoperative X-ray
Five days later, due to persistent abdominal distension and dark bilious discharge via an orogastric tube, he underwent a second opera- tion. During the second laparotomy, dehiscence of the previous anastomosis and dilation of the descending colon containing intestinal contents were observed. As the diagnosis of the malfor- mation had not been established initially and there was a previous colonic perforation, it was decided to perform a double-outlet diverting

Figure 2. Rectal atresia on physical examination
colostomy, utilising the previous surgical site. The proximal stump (ascending colon) and the distal stump (descending colon) were brought out on opposite flanks, allowing for effective diversion without the need for further resection or anastomosis. Although this type of procedure does not correspond to the usual location in the lower left quadrant, it was considered the safest option given the local conditions. The distal segment was irrigated with saline solution, with no discharge through the anal canal, confirming the diagnosis of previously unrecognised rectal atresia. The procedure was completed with peritoneal lavage. The patient was transferred to the neonatal intensive care unit, where he remained intubated and on mechanical venti- lation for three days.
The colostomy was functional 12 hours after the end of surgery. On the third postoperative day, the patient was extubated and enteral feeding was restarted with good tolerance. He completed a course of antibiotics with pipera- cillin/tazobactam and metronidazole. During hospitalisation, additional imaging studies were performed to rule out associated malformations; for instance, spinal canal ultrasound showed no abnormalities suggestive of tethered cord, and upper and lower abdominal ultrasound revealed kidneys with normal morphology and echoge- nicity, without urinary tract dilation or presacral masses. On the fifth postoperative day, the patient was discharged due to an appropriate clinical course.
At 6 months of age, a contrast study via a distal colostomy was performed, ruling out fis- tulas into the urinary tract and confirming rectal atresia (Figure 3). Subsequently, a recto-anal anastomosis was performed via a posterior sag- ittal approach with preservation of the anal canal (Figure 4), following the technique described by Peña et al. [8], which allows for complete exposure of the sphincteric complex and precise anatomical reconstruction of the recto-anal ca- nal. During the procedure, a type I rectal atresia was identified according to the classification by
Oliveros-Rivero J., Fajardo-Ponce G.
Congenital rectal atresia: a rare malformation that may go unnoticed. Case report.
Arch Med (Manizales). 2026;26(1)

Figure: 3a. AP view of the distal cologram; 3b. Lateral view of the distal cologram.
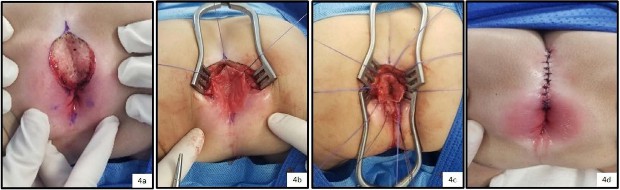
Figure: 4a. PSAP incision; 4b. Rectal atresia; 4c. opening of the rectum and start of the end-to-end anastomosis; 4d. surgery completed
Peña and De Vries (1982), characterised by the presence of a fibrous septum approximately 1 cm in length separating the proximal and distal segments, both of similar calibre and with ad- equate blood supply. This finding corresponds to the septal or membranous variant, which allowed a direct end-to-end anastomosis to be performed without the need for intestinal taper- ing. A biopsy of the distal colon was taken for
histopathological examination, which revealed the presence of normal ganglion cells, ruling out Hirschsprung’s disease. The patient began feeding 12 hours postoperatively, completed a course of antibiotics with ceftriaxone and amikacin, and was discharged on the seventh day. Outpatient follow-up included the use of Hegar dilators for anal dilation according to the age-specific protocol.
Oliveros-Rivero J., Fajardo-Ponce G.
Congenital rectal atresia: a rare malformation that may go unnoticed. Case report.
Arch Med (Manizales). 2026;26(1)
Finally, after completing the course of anal dilations with Hegar dilators as recommended in the literature [9] and confirming the absence of stenosis by digital rectal examination, it was decided not to perform the distal cologram. At 11 months of age, an exploratory laparotomy was performed to close the colostomy, with a latero-lateral anastomosis of the transverse colon using a mechanical stapler and place- ment of a Blake drain. The patient resumed oral intake on the fourth postoperative day and had bowel movements via the anus on the fifth day. The drain was removed on the seventh day, and the patient was discharged on the eighth day with outpatient follow-up at 1, 3 and 6 months, showing good clinical and functional progress.
this case demonstrates how an incomplete initial clinical assessment can lead to diagnostic delays in rare neonatal conditions such as rectal atresia. Despite the presence of classic symp- toms such as abdominal distension, vomiting and failure to pass meconium, the finding of a normal-appearing anus led to a misdiagnosis of necrotising enterocolitis. The case reaffirms that the neonatal physical examination should include not only perineal inspection, but also verification of anal patency using appropriate instruments [1–3,10].
Most cases of rectal atresia in the literature present in the neonatal period, with difficulty passing a thermometer or dilator beyond 1.5–2 cm from the anal margin [2,6,11]. As in our patient, the normal appearance of the anus delays diagnosis until complications such as colonic perforation become evident or a lack of clinical improvement with medical manage- ment is observed. Furthermore, it has been reported that a diversion colostomy not only allows for decompression but also facilitates
contrast studies that confirm the absence of fistulas [6,7].
Regarding the surgical approach, multiple techniques have been described: posterior sagittal anorectoplasty, transanal anastomosis, laparoscopically assisted anastomosis, and other less common techniques such as mag- netic compression anastomosis [5,6,12,13]. Although there is no universal consensus, the primary objective is to preserve the sphincter apparatus and achieve functional continence. In our experience, the staged technique al- lowed for stabilisation, accurate diagnosis, and reconstruction with good clinical and functional outcomes, which is consistent with reports in the literature [5,6,11].
This clinical case contributes to the literature by highlighting the importance of timely diagno- sis of this rare condition, as well as the value of a staged surgical approach in experienced centres. Correct identification of cases with a normal anus should lead to the exclusion of rec- tal atresia when there is low-level obstruction, and paediatric surgeons should be familiar with the various repair techniques and their selec- tion based on the anatomical characteristics of each patient.
A comparison of our case with previously published reports is summarised in Table 1.
congenital rectal atresia is a rare malforma- tion that can go undetected in the presence of a normal-appearing anus. Early diagnosis through careful physical examination and a staged surgical approach can prevent compli- cations and lead to good functional outcomes.
Oliveros-Rivero J., Fajardo-Ponce G.
Congenital rectal atresia: a rare malformation that may go unnoticed. Case report.
Arch Med (Manizales). 2026;26(1)
No. | Author / Year | Age at the time of surgery | Sex | Weight at the time of surgery | Previous colostomy | Surgical technique | Outcome |
1 | Laamrani et al, 20143 | 20 days | F | - | No | ATT- ARSP | Good |
2 | Hamid et al, 20224 | 3 months | M | 2.5 kg | Yes | ATT- ARSP | Good |
3 months | M | 3 kg | Yes | ATT- ARSP | Good | ||
1 day | F | 3 kg | Yes | ATT- ARSP | Good | ||
3 | from Beaufort et al, 20235 | 70 patients (1 day to 6 years of age) | M (n=37) F(n=21) N/A (n=12) | N/E | Yes (n=56) No (n=14) | ATT- ARSP (n=43) DTA (n=18) Local resection (n=8) Magnamosis (n=1) | Good (n=66) Poor (n=4) |
4 | Shehata et al, 20236 | 6 months | M | - | Yes | ART | Good |
6 months | M | - | Yes | ART | Good | ||
6 months | M | - | Yes | ART | Good | ||
6 months | F | - | Yes | ART | Good | ||
5 | by Beaufort et al, 20237 | 18 patients 2–6 months (median 5 months) | M (n=10) F(n=8) | N/A | Yes (n=16) No (n=2) | ATT- ARSP (n=9) DTA (n=1) ART (n=1) ACR (n=1) ATA + D (n=1) N/A (n=5) | Good (n=11) Poor (n=2) Died before surgery (n=1) N/A (n=4) |
6 | Sharma et al, 20178 | 1 day | N/A | - | Yes | DAP | Good |
1 day | N/A | - | Yes | DAP | Good | ||
1 day | N/A | - | Yes | ATT- ARSP | Good | ||
1 day | N/A | - | Yes | ATT- ARSP | Good | ||
1 day | N/A | - | Yes | ATO - ARSP | Good | ||
7 | Gieballa et al, 20189 | 7 months | M | - | Yes | DTA | Good |
6 months | M | - | Yes | DTA | Good | ||
10 months | M | - | Yes | DTA | Good | ||
8 | Jiang et al, 202410 | 5 months | F | - | Yes | DTA | Good |
9 | Mehmetoğlu et al, 201811 | 9 months | M | - | Yes | ATT- ARSP | Good |
10 | Dias et al, 198214 | 12 months | M | - | Yes | ATT-ASU | Good |
11 | Upadhyaya, 199015 | 42 months | M | - | Yes | ART | Good |
6 months | M | - | Yes | ART | Good | ||
12 | Kisra et al, 200516 | 3 months | M | - | Yes | ATT- ARSP | Mild stenosis resolved with dilation |
3 months | M | - | Yes | ATT- ARSP | Mild stenosis resolved with dilation | ||
3 months | M | - | Yes | ATT- ARSP | Good | ||
3 months | M | - | Yes | ATT- ARSP | Good | ||
13 | Nguyen TL et al, 200717 | 3 months | F | 2.3 kg | Yes | ART-LA | Good |
3 months | F | 2.7 kg | Yes | ART-LA | Good | ||
14 | Hamrick et al, 201218 | 17 patients (aged 2 days to 6 years) | M(n=10) F(n=7) | - | Yes (n=13) No (n=4) | ATT- ARSP (n=4) ATO- ARSP (n=13) | Good, 5 patients (29%) with mild constipation |
15 | Our case | 4 months | M | 5.1 kg | Yes | ATT- ARSP | Good |
ATT-ARSP: End-to-end anastomosis following posterior sagittal anorectoplasty; ART: Transanal rectoanal anastomosis; DAP: Abdominoperineal approach; N/E: Not specified; DTA: Transanal endorectal approach; ACR: Colorectal anastomosis; ATA + D: Transanal opening under anaesthesia
+ dilation; ATO-ARSP: End-to-oblique anastomosis following posterior sagittal anorectoplasty; ATT-ASU (End-to-end anastomosis via single sacral approach); ART-LA: Laparoscopically assisted transanal rectoanal anastomosis.
Oliveros-Rivero J., Fajardo-Ponce G.
Congenital rectal atresia: a rare malformation that may go unnoticed. Case report.
Arch Med (Manizales). 2026;26(1)
Lane VA, Wood RJ, Reck C, Skerritt C, Levitt MA. Rectal atresia and anal stenosis: the difference in the opera- tive technique for these two distinct congenital anorectal malformations. Tech Coloproctol. 2016; 20(4): 249-54. https://doi.org/10.1007/s10151-016-1435-5
Al-Salem AH. Congenital Rectal Stenosis and Atresia. In: Atlas of Paediatric Surgery: Principles and Treatment. Springer; 2020. Chapter 55. https://doi.org/10.1007/978-3-030-29211-9_55
Laamrani FZ, Dafiri R. Rectal atresia: a rare cause of failure to pass meconium. Pan Afr Med J. 2014; 19:198. https://doi.org/10.11604/pamj.2014.19.198.4057
Hamid R, Ahmad S, Bhat N. Rectal atresia: an uncommon entity: Experience of three cases. J Neonatal Surg. 2022;11:28. Available at: https://pdfs.semanticscholar.org/6e54/d64908b5f37db3c8eeb6f13f8726e4c24b57.pdf
de Beaufort CMC, Derikx JPM, de Jong JR, Burchell GL, Bosscha SRJ, de Beer SA, et al. Outcomes after Surgi- cal Treatment for Rectal Atresia in Children: Is There a Preferred Approach? A Systematic Review. Eur J Pediatr Surg. 2023;33(5):345-353. https://doi.org/10.1055/s-0042-1758152
Shehata S, ElSawaf M, Kotb M. Transanal recto-anal anastomosis for treatment of rectal atresia: a review of 4 cases. BMC Paediatr. 2023;23(1):46. https://doi.org/10.1186/s12887-023-03859-9
de Beaufort CMC, Gorter RR, Iacobelli BD, Midrio P, Sloots CEJ, Samuk I, et al. Rectal atresia and rectal stenosis: the ARM-Net Consortium experience. Pediatr Surg Int. 2023;39(1):242. https://doi.org/10.1007/s00383-023-05518-7
Peña A, DeVries PA. Posterior sagittal anorectoplasty: important technical considerations and new applications. J Pediatr Surg. 1982; 17(6):796-811. https://doi.org/10.1016/s0022-3468(82)80448-x
Levitt MA, Peña A. Anorectal malformations. Orphanet J Rare Dis. 2007; 26;2:33. https://doi.org/10.1186/1750-1172-2-33
Sharma S, Gupta DK. Varied facets of rectal atresia and rectal stenosis. Pediatr Surg Int. 2017;33(8):829-836. https://doi.org/10.1007/s00383-017-4106-3
Gieballa M, AlKharashi N, Al-Namshan M, AlJadaan S. Outcomes of transanal endorectal pull-through for rectal atresia. BMJ Case Reports. 2018;2018:bcr2017224080. https://doi.org/10.1136/bcr-2017-224080
Jiang G, Wu L, Ruan W, Zhu J. Congenital rectal atresia: a case report. Asian J Surg. 2024;47(8):3796–3797. https://doi.org/10.1016/j.asjsur.2024.04.133
Mehmetoğlu F. Rectal Atresia and Congenital Hypothyroidism: An Association or Coincidence? European J Pediatr
Surg Rep. 2018;6(1):e7-e10. https://doi.org/10.1055/s-0037-1612610
Dias RG, Santiago AP, Ferreira MC. Rectal atresia: treatment through a single sacral approach. J Pediatr Surg. 1982;17(4):424-425. https://doi.org/10.1016/S0022-3468(82)80506-X
Upadhyaya P. Rectal atresia: transanal, end-to-end, rectorectal anastomosis – a simplified, rational approach to management. J Pediatr Surg. 1990;25(5):535-537. https://doi.org/10.1016/0022-3468(90)90567-S
Kisra M, Alkadi H, Zerhoni H, Ettayebi F, Benhammou M. Rectal atresia. J Paediatr Child Health. 2005;41(12):691- 693. https://doi.org/10.1111/j.1440-1754.2005.00763.x
Nguyen TL, Pham DH. Laparoscopic and transanal approach for rectal atresia: a novel alternative. J Pediatr Surg. 2007;42(11):E25-E27. https://doi.org/10.1016/j.jpedsurg.2007.08.049
Hamrick M, Eradi B, Bischoff A, Louden E, Peña A, Levitt MA. Rectal atresia and stenosis: unique anorectal malformations. J Pediatr Surg. 2012;47(6):1280-1284. https://doi.org/10.1016/j.jpedsurg.2012.03.036
![]()