Effect of strength training in young people with Down Syndrome: a systematic review
Yann Vinicius de Brito Santos Silva1, Giullio César Pereira Salustiano Mallen da Silva2,
Alex Santos Meireles3, Diego Gama Linhares4, Ravini de Souza Sodré5,
Ana Beatriz Moreira de Carvalho Monteiro6, Dirceu Ribeiro Nogueira da Gama7,
Rodrigo Gomes de Souza Vale8.
Recibido para publicación: 29-02-2024. Versión corregida: 24-04-2024. Aprobado para publicación: 27-06-2024.
Modelo de citación:
Brito Santos Silva Y.V., Pereira Salustiano Mallen da Silva G.C., Santos Meireles A., Gama Linhares D. Souza Sodré R., Moreira de Carvalho Monteiro A.B., Nogueira da Gama D.R., Gomes de Souza Vale R. Effect of strength training in young people with Down Syndrome: a systematic review. Arch Med (Manizales). 2024;24(2). https://doi.org/10.30554/archmed.24.2.5079.2024
Abstract
Background: Down syndrome is a condition caused by a genetic anomaly that affects the physical and intellectual development of individuals. A significant number adopt a sedentary lifestyle, potentially due to such health conditions or lack of guidance and support from healthcare and fitness professionals. Objective: To analyze the effects of strength training in young individuals with Down Syndrome. Methods: This systematic review was conducted following the recommendations outlined by PRISMA and was registered on the PROSPERO platform (CRD42024501671). The PICOS acronym was used to define the eligibility criteria. The databases searched included MEDLINE (PubMed), Scopus, and Web of Science using the following phrases: (((resistance training [Title/Abstract]) OR (strength training [Title/Abstract])) AND (down syndrome [Title/Abstract])) OR (Trisomy 21 [Title/Abstract]). Results: A total of 911 articles were retrieved. Following screening, three randomized clinical trials meeting the specified criteria were included in the analysis, comprising 114 participants, with 57 in each group. The included articles were deemed to have a low risk of bias according to the RoB 2.0 tools and achieved a minimum score of 12 points on the TESTEX tool. Conclusions: Strength training can significantly improve muscle strength in children and young individuals with Down syndrome by promoting functional independence and social integration.
Keywords: Down syndrome, strength training, physical exercise, trisomy of chromosome 21.
Efecto del entrenamiento de fuerza en jóvenes con síndrome de Down: una revisión sistemática
Resumen
Antecedentes: El síndrome de Down es una enfermedad causada por una anomalía genética que afecta al desarrollo físico e intelectual de los individuos. Un número significativo adopta un estilo de vida sedentario, potencialmente debido a dichas condiciones de salud o a la falta de orientación y apoyo por parte de los profesionales de la salud y del ejercicio físico. Objetivo: Analizar los efectos del entrenamiento de fuerza en individuos jóvenes con síndrome de Down. Métodos: Esta revisión sistemática se realizó siguiendo las recomendaciones marcadas por PRISMA y se registró en la plataforma PROSPERO (CRD42024501671). Se utilizó el acrónimo PICOS para definir los criterios de elegibilidad. Las bases de datos buscadas incluyeron MEDLINE (PubMed), Scopus y Web of Science utilizando las siguientes frases: (((entrenamiento de resistencia [Título/Abstract]) OR (entrenamiento de fuerza [Título/Abstract]) AND (síndrome de down [Título/Abstract])) OR (Trisomía 21 [Título/Abstract]). Resultados: Se recuperó un total de 911 artículos. Tras el cribado, se incluyeron en el análisis tres ensayos clínicos aleatorizados que cumplían los criterios especificados, con 114 participantes, 57 en cada grupo. Se consideró que los artículos incluidos tenían un bajo riesgo de sesgo según las herramientas RoB 2.0 y alcanzaron una puntuación mínima de 12 puntos en la herramienta TESTEX. Conclusiones: El entrenamiento de fuerza puede mejorar significativamente la fuerza muscular en niños y jóvenes con síndrome de Down promoviendo la independencia funcional y la integración social.
Palabras clave: Síndrome de Down, entrenamiento de fuerza, ejercicio físico, trisomía del cromosoma 21.
Efeito do treinamento de força em jovens com síndrome de Down: uma revisão sistemática
Resumo:
Histórico: A síndrome de Down é uma condição causada por uma anomalia genética que afeta o desenvolvimento físico e intelectual dos indivíduos. Um número significativo de pessoas adota um estilo de vida sedentário, possivelmente devido a essas condições de saúde ou à falta de orientação e apoio de profissionais de saúde e de condicionamento físico. Objetivo: Analisar os efeitos do treinamento de força em indivíduos jovens com Síndrome de Down. Métodos: Essa revisão sistemática foi realizada seguindo as recomendações descritas pelo PRISMA e foi registrada na plataforma PROSPERO (CRD42024501671). O acrônimo PICOS foi usado para definir os critérios de elegibilidade. Os bancos de dados pesquisados incluíram MEDLINE (PubMed), Scopus e Web of Science usando as seguintes frases: (((resistance training [Title/Abstract]) OR (strength training [Title/Abstract])) AND (down syndrome [Title/Abstract])) OR (Trisomy 21 [Title/Abstract]). Resultados: Um total de 911 artigos foi recuperado. Após a triagem, três ensaios clínicos randomizados que atendiam aos critérios especificados foram incluídos na análise, compreendendo 114 participantes, com 57 em cada grupo. Os artigos incluídos foram considerados como tendo baixo risco de viés de acordo com as ferramentas RoB 2.0 e atingiram uma pontuação mínima de 12 pontos na ferramenta TESTEX. Conclusões: O treinamento de força pode melhorar significativamente a força muscular em crianças e jovens com síndrome de Down, promovendo a independência funcional e a integração social.
Palavras-chave: Síndrome de Down, treinamento de força, exercício físico, trissomia do cromossomo 21.
Introduction
Down syndrome is a condition caused by a genetic anomaly that affects the physical and intellectual development of individuals. Many of these individuals are born or develop health conditions that compromise their quality of life. A significant number adopt a sedentary lifestyle, potentially due to such health conditions or the lack of guidance and support from healthcare and fitness professionals [1].
Physical activity levels in individuals with Down syndrome tend to be lower and often decrease over time, which may contribute to higher rates of metabolic disease and obesity. Additionally, they commonly present musculoskeletal alterations, low stature, irregularities in bone density, ligament laxity, and delayed development of motor and cognitive function [2,3].
Motor development progression in children with Down syndrome occurs parallel to that in children without disabilities, albeit at a slower pace. This was attributed to the increased risk of premature sarcopenia and the presence of generalized hypotonia, muscle weakness, and joint hyperflexibility. Therefore, the limited ability to perform activities of daily living and engage regularly in physical exercise during childhood can potentially lead to inadequate neuromuscular development [4,5]. Hence, encouraging and maintaining regular exercise practices is an important strategy for the care and support of the Down syndrome population [6].
Strength training is a form of physical exercise with the potential to reduce muscle strength loss, improve body composition, and enhance functional capacity in young and adult individuals with Down syndrome. Improvements in muscle strength have been linked to beneficial effects, especially in functional activities, which contribute to advancements in physical fitness. Furthermore, the effects of training are not limited solely to physical aspects but also extend to autonomy, quality of life, and social inclusion [4,7].
It is possible to observe in the literature some exercise methods practiced with the aim of improving the strength production capacity of individuals with Down syndrome, such as progressive resistance training (twice a week for ten weeks, two to three sets of 10 to 12 repetitions of each exercise until failure) [8], strength and agility training (three times a week for 6 weeks, 5 minutes of treadmill exercise, and 20 minutes of virtual-reality based activity) [9], or Wii-based training programs (three times a week, 1 h sessions, using the Wii Fit Balance Board) [10]. Thus, considering the benefits and importance of understanding interventions for this population, the present systematic review aimed to analyze the effects of strength training in children and young individuals with Down syndrome.
Methods
Study design
This study is a systematic review drafted in accordance with the guidelines recommended by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [11]. A search was conducted using PROSPERO, where no reviews on specific topics were found. The study was registered under registration number CRD42024501671.
Eligibility criteria
The studies included in this review followed the PICOS acronym [12]: population (P): young individuals with Down syndrome; intervention (I): traditional strength training; comparison (C): control group; outcome (O): strength variable, and study design (S): randomized clinical trials. Articles with other methodological designs were excluded, as were studies involving individuals over 18 years of age.
Search strategy
In January 2024, a search was conducted exclusively using filters for randomized clinical trials in the MEDLINE (PubMed), Scopus, and Web of Science databases, using the following search phrase: (((resistance training [Title/Abstract]) OR (strength training [Title/Abstract])) AND (down syndrome [Title/Abstract])) OR (Trisomy 21[Title/Abstract]) (Appendix 1). After the search, all references found were imported into EndNote software, which three independent reviewers had access to. Two reviewers were responsible for removing duplicates and reviewing titles and abstracts, followed by analysis of full-text articles. The third reviewer resolved any discrepancies in the decisions made during the process.
Methodological quality assessment
Methodological quality was assessed using the Tool for the Assessment of Study Quality and Reporting in Exercise (TESTEX), which was designed to evaluate the quality of studies and reports in the context of physical exercise. TESTEX consists of a scale comprising 15 points, specifically developed for experimental studies, encompassing criteria that assess internal validity and the presentation of statistical analysis. Each criterion on the scale is scored with one point, whereas the absence of these indicators results in zero points. The maximum achievable score is 15. The scale included the following criteria: 1) specification of inclusion criteria; 2) random allocation; 3) allocation concealment; 4) similarity of groups at baseline; 5) blinding of assessor (for at least one key outcome); 6) measurement of at least one primary outcome in 85% of allocated subjects (up to three points); 7) intention-to-treat analysis; 8) between-group comparison of at least one primary outcome (up to two points); 9) reporting measures of variability for all reported outcome measures; 10) monitoring of activities in control groups; 11) relative exercise intensity remained constant; and 12) characteristics of exercise volume and energy expenditure[13].
Assessment of bias risk
The Risk of Bias 2.0 (RoB 2.0) tool was employed to assess bias risk. RoB 2.0 is a tool developed to assist in the critical evaluation process of studies in systematic reviews, allowing reviewers to examine the risk of bias in individual studies included in the review. This tool addresses multiple domains of bias, each focusing on a specific area of study design. The domains assessed by RoB 2.0 includes: 1. Selection Bias: Refers to how participants were selected for comparison; 2. Performance Bias: Evaluates the presence of bias due to systematic differences between groups in the administration of the intervention; 3. detection bias: related to the presence of bias due to systematic differences between groups in outcome measurement; 4. Attribution Bias: Refers to how results are attributed to participants; 5. Reporting Bias: Assesses whether results are reported fully and accurately[14].
Data extraction
Data from the selected articles were independently extracted by two assessors. In cases of disagreement, a third assessor was consulted for a final decision. For sample characterization, the following data were collected: year of publication, country of origin of the article, number of participants, age, total body mass, height, and intelligence quotient (IQ). Additionally, data related to the proposed intervention in each article were extracted as follows: type of intervention, exercise used, intervention duration, weekly frequency, volume, intensity, and outcomes.
Results
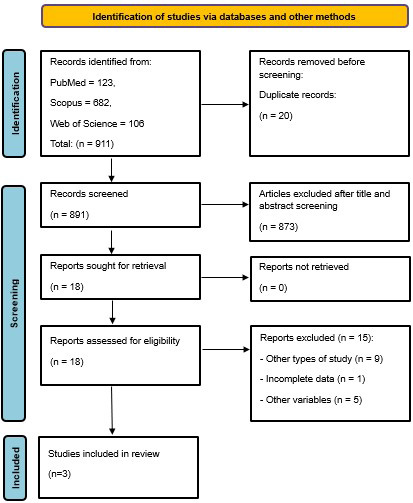
Based on previously established criteria, 911 articles were retrieved (PubMed = 123, Scopus = 682, Web of Science, 106). Of these, 20 were identified as duplicates and 873 were excluded after title and abstract evaluation. Subsequently, 14 articles were excluded during full-text reading, resulting in 3 articles [15-17] that met the inclusion criteria (Figure 1).
The characteristics of the sample are presented in Table 1. Of the three selected articles, one was from India [15], and the other two were from Australia [16,17]. The total number of participants was 144, who were divided into a control group (n=57) and an experimental group (n=57). The mean age of the control group was 15.5 years and that of the experimental group was 15.7 years. Only one study [15] provided participants’ intelligence quotient. All the studies included participants of both sexes.
Table 1. Descriptive characteristics of the included studies
|
Author and year of publication |
Country |
Control Group |
Experimental Group |
|
Gupta et al., 2010[15] |
India |
n: 11; |
n: 12; |
|
Shields e Taylor, 2010[16] |
Australia |
n: 12; |
n: 11; |
|
Shields et al., 2013[17] |
Australia |
n: 34; |
n: 34; |
|
Legend: n= sample size; M= male; F= female; TBM= total body mass; BMI= body mass index; IQ= intelligence quotient; NI= not informed. |
|||
Table 2 presents the data extracted from the interventions conducted in the selected studies with the combination of volume, intensity, and interval of the proposed stimuli. Only one study [15] used a dynamometer to assess participants’ force production capacity, while the other two studies [16,17] used one-repetition maximum (1RM) testing for this evaluation. All three studies [15-17] presented training models with load progression over the intervention weeks. Two studies [16,17] had a minimum weekly frequency of two training sessions and conducted their interventions for 10 weeks (total of 20 sessions), while the other [15] used three weekly sessions, but over six weeks of intervention (total of 18 sessions).
The methodological quality of the included studies is shown in Table 3. Two Articles [16,17] scored 15 points, the maximum possible score achievable by the TESTEX tool, whereas another study [15] scored 13 points. Additionally, the risk of bias can be observed in figure 2 through RoB 2.0, where all three articles exhibited a low risk of bias in all analyzed criteria.
Table 2. Data extracted from the included studies
|
Author/Year |
Intensity |
Duration/Volume |
WF |
W |
Exercises |
Assessment |
Results |
|
Gupta et al., 2010[15] |
Starting at 50%. 0.5 kg progression based on the ease demonstrated in the exercise. |
2 x 10 reps per muscle group. |
3 |
6 |
Exercises with sandbags |
Dynamometer |
- Hip flexion: ↑ |
|
Shields e Taylor, 2010[16] |
Progressive based on the ease demonstrated in the exercise. |
3 x 12 reps of each exercise or to concentric muscular failure.
|
2 |
10 |
Upper limbs: |
1RM test: |
- 1RM Leg Press: ↑ |
|
60%-80% of 1RM, with progression based on the capability to perform 3 x 12 reps of the exercise. |
3 x 12 reps of each exercise or to concentric muscular failure. 2 minutes of rest interval. |
2 |
10 |
Upper limbs: |
1RM test: |
Post-intervention: |
|
|
Legend: WF= weekly frequency; W= intervention duration in weeks; 1RM= one maximum repetition; reps= repetitions; Ext= extension; Flex= flexion; Abd= abduction; Seat= seated; ↑= improvement post-intervention compared to the control group; ↔= no post-intervention difference compared to the control group. |
|||||||
Table 3. Analysis of methodological quality using the TESTEX tool
|
Studies |
1 |
2 |
3 |
4 |
5 |
Partial (0 a 5) |
6a |
6b |
6c |
7 |
8a |
8b |
9 |
10 |
11 |
12 |
Partial (0 a 10) |
Total (0 a 15) |
|
Gupta et al., 201015 |
1 |
1 |
1 |
1 |
0 |
4 |
1 |
0 |
1 |
1 |
1 |
1 |
1 |
1 |
1 |
1 |
9 |
13 |
|
1 |
1 |
1 |
1 |
1 |
5 |
1 |
1 |
1 |
1 |
1 |
1 |
1 |
1 |
1 |
1 |
10 |
15 |
|
|
Shields et al., 201317 |
1 |
1 |
1 |
1 |
1 |
5 |
1 |
1 |
1 |
1 |
1 |
1 |
1 |
1 |
1 |
1 |
10 |
15 |
Legend: *: studies that did not report the number of dropouts, but all ended with the same number of participants who started the intervention; NC: no control group. Study quality: 1 = specific eligibility criteria, 2 = specified randomization type, 3 = allocation concealment, 4 = similar groups at baseline, 5 = assessors were blinded (at least for one main outcome); 6 = outcomes assessed in 85% of participants (6a = 1 point if more than 85% completed; 6b = 1 point if adverse events were reported; 6c = if exercise adherence was reported); 7 = intention-to-treat statistical analysis; 8 = statistical comparison between groups (8a = 1 point if group comparisons were reported for the primary outcome variable of interest; 8b = 1 point if statistical comparisons between groups were reported for at least one secondary measure); 9 = point estimates and variability measures for all reported outcome measures; 10 = activity monitoring in the control group; 11 = relative exercise intensity remained constant; 12 = exercise volume and energy expenditure were reported.

Fig. 2. Analysis of bias risk using RoB 2.0 tools.
Discussion
This systematic review aimed to analyze the effects of strength training in children and young individuals with Down syndrome. Although the benefits that resistance training can provide for this population seem clear, few randomized clinical trials addressing the effects of resistance training in young people with Down syndrome were found in the searches conducted. Nevertheless, three studies found [15-17] provided relevant information regarding the impact of these specific interventions.
In one study [15], a substantial improvement in lower limb muscle strength was noted after the intervention. The gradual progression adapted to individual capacity demonstrated during exercises proved to be a key element for the success of the training program. The diversity of exercises, including hip flexion, hip abduction, and knee extension, was effective in promoting strength gain in the muscle groups stimulated by these exercises. Furthermore, the study demonstrated a significant increase in participants’ balance. These findings are consistent with another study [18], which reported that low levels of balance in young individuals with Down syndrome can result in motor delays and impairments as well as increase the risk of falls.
On the other hand, another study [16] adopted a progressive approach to adapt intensity and volume according to the individual capacity of young individuals with Down syndrome. During the study, participants performed a variety of exercises for both the lower and upper limbs, with special focus on the latissimus dorsi muscle. The results indicated improvements in lower-limb muscle strength, as evidenced by the 1RM test in the leg press exercise. However, no changes were observed in the upper limb muscle strength in the 1RM test performed in the seated bench press exercise. Additionally, it was hypothesized that the emphasis on exercises for the latissimus dorsi may be related to improved postural control in young individuals with Down syndrome. This hypothesis is supported by a study [19] that indicated a deficit in postural control in individuals with Down syndrome. The authors attributed these findings to musculoskeletal characteristics inherent to ligament laxity and hypotonia, either directly or indirectly.
A previous study [17] reported findings regarding strength training for young individuals with Down syndrome. The authors employed progressive loads based on individuals’ capacity to perform three sets of 12 repetitions, with the intensity increasing from 60% to 80% of 1RM. Following the intervention, the results demonstrated increased muscle strength in both the lower and upper limbs, as indicated by the 1RM tests in the leg press and seated bench press exercises. However, at three months post-intervention, only the lower limbs maintained muscle strength.
The results of the study [17] indicated an increase in upper limb muscle strength compared with the findings of another study [16]. One hypothesis is that the frequency of load progression during the intervention was sufficient to reach or approach an intensity between 60 and 80% of 1RM. This hypothesis is supported by a study [20] that demonstrated that moderate loads between 60 and 79% of 1RM can be equivalent to 8 and 15RM. Similarly, a study [21] reinforced that gains in muscle strength are considerably higher with high-load training (>60% of 1RM) than with lower loads (<60% of 1RM).
After analyzing the results of the studies included in this systematic review, it is recommended that a training program for individuals with Down syndrome be conducted with a minimum frequency of 2–3 times per week, consisting of 2–3 sets of 10–12 repetitions. The training intensity should be progressively increased, considering the ease of execution demonstrated during exercises, which appears to be a safe approach for increasing muscle strength. Moderate loads between 60 and 80% of 1RM or repetitions between 8 and 15RM seem to be safe for training. Additionally, exercise prescription and selection should be based on the specific needs of individuals with Down syndrome.
Some limitations were observed in the present study, such as the small number of articles analyzed, although with good methodological quality and a low risk of bias. Another limitation relates to the publication year, with production dates between 2010 and 2013. Additionally, only one article provided information on the participants’ IQ, as cognitive capacity can influence their ability to understand and perform the proposed exercises.
Conclusion
The studies analyzed in this systematic review highlighted that strength-training programs had a positive impact on upper and lower limb muscle strength in children and young individuals with Down syndrome. These findings expand our understanding of the effects of physical exercise on the health and well-being of people with Down and provide guidelines for prescribing strength training. Thus, strength training can be a strategy to improve functional independence and facilitate participation in daily activities and can be included as an integral part of multidisciplinary intervention programs aimed at the health and overall development of these individuals. These aspects can contribute to inclusion and social integration.
It is recommended for future studies to investigate the effects of resistance training on strength production and other parameters such as static and dynamic balance, as well as motor coordination in the population under consideration.Parte superior do formulário
Conflicts of interest´
We declare that there are no financial, personal, or institutional conflicts of interest regarding the information and results disclosed in this manuscript.
References
1. Boer PH. The effect of 8 weeks of freestyle swim training on the functional fitness of adults with Down syndrome. J Intellect Disabil Res. 2020; 64(10): 770-781. doi:10.1111/jir.12768.
2. Post EM, et al. The Effects of Resistance Training on Physical Fitness and Neuromotor-Cognitive Functions in Adults with Down Syndrome. Front Rehabil Sci. 2022; 3: 927629. doi:10.3389/fresc.2022.927629.
3. Melo JEB, Silva SMP, Barros GWP. The importance of physical activity for children with Down syndrome. Braz J Dev. 2021; 7(11): 103202-103213. doi:10.34117/bjdv7n11-101.
4. Balensiefer MD, et al. Melhora das habilidades motoras após treinamento funcional: estudo de caso com um indivíduo portador de síndrome de Down. Rev Foco. 2023; 16(11): e3385. doi:10.54751/revistafoco.v16n11-050.
5. Sugimoto D, et al. Effects of Neuromuscular Training on Children and Young Adults with Down Syndrome: Systematic Review and Meta-Analysis. Res Dev Disabil. 2016; 55: 197-206. doi:10.1016/j.ridd.2016.04.003.
6. Diaz AJ, et al. Effects of Resistance Training in Muscle Mass and Markers of Muscle Damage in Adults with Down Syndrome. Int J Environ Res Public Health. 2021; 18(17): 8996. doi:10.3390/ijerph18178996.
7. Melo GLR, et al. Resistance training and Down Syndrome: A narrative review on considerations for exercise prescription and safety. Front Physiol. 2022; 13: 948439. doi:10.3389/fphys.2022.948439.
8. Shields N, Taylor NF, Dodd KJ. Effects of a community-based progressive resistance training program on muscle performance and physical function in adults with Down syndrome: a randomized controlled trial. Arch Phys Med Rehabil. 2008; 89: 1215–1220. doi: 10.1016/j.apmr.2007.11.056.
9. Lin HC, Wuang YP. Strength and agility training in adolescents with Down syndrome: a randomized controlled trial. Res Dev Disabil. 2012; 33: 2236–2244. doi: 10.1016/j.ridd.2012.06.017.
10. Silva V, et al. Wii-based exercise program to improve physical fitness, motor proficiency and functional mobility in adults with Down syndrome. J Intell Disabil Res. 2017; 61: 755–756. doi: 10.1111/jir.12384.
11. Sarkis-Onofre R, et al. How to properly use the PRISMA Statement. Syst Rev. 2021; 10(1): 1-3. doi:10.1186/s13643-021-01671-z.
12. Tocchio dos Anjos N de S, Portilho BCR. Elaboração da pergunta de pesquisa. In: Mendonça AVM, Sousa MF, editors. Métodos e técnicas de pesquisa qualitativa em saúde. Vol. 1. Brasília, DF: ECoS; 2021.
13. Smart NA, et al. Validation of a new tool for the assessment of study quality and reporting in exercise training studies: TESTEX. Int J Evid Based Healthc. 2015; 13(1): 9-18. doi:10.1097/xeb.0000000000000020.
14. Sterne JAC, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019; 366. doi:10.1136/bmj.l4898.
15. Gupta S, Rao BK, Kumaran SD. Effect of strength and balance training in children with Down’s syndrome: a randomized controlled trial. Clin Rehabil. 2010; 25(5): 425-432. doi:10.1177/0269215510382929.
16. Shields N, Taylor NF. A student-led progressive resistance training program increases lower limb muscle strength in adolescents with Down syndrome: a randomised controlled trial. J Physiother. 2010; 56(3): 187-193. doi:10.1016/s1836-9553(10)70024-2.
17. Shields N, et al. A community-based strength training programme increases muscle strength and physical activity in young people with Down syndrome: A randomised controlled trial. Res Dev Disabil. 2013; 34(12): 4385-4394. doi:10.1016/j.ridd.2013.09.022.
18. Jung HK, Chung EJ, Lee BHA. Comparison of the balance and gait function between children with Down syndrome and typically developing children. J Phys Ther Sci. 2017; 29(1): 123-127. doi:10.1589/jpts.29.123.
19. Guzman-Muñoz EE, Gutierrez-Navarro LB, Miranda-Diaz SE. Postural control in children, adolescents and adults with Down syndrome. Int Med Rev Down Syndr. 2017; 21(1): 12-16. doi:10.1016/j.sdeng.2016.09.003.
20. Carvalho L, et al. Muscle hypertrophy and strength gains after resistance training with different volume-matched loads: a systematic review and meta-analysis. Appl Physiol Nutr Metab. 2022;47(4). doi:10.1139/apnm-2021-0515.
21. Schoenfeld BJ, et al. Strength and hypertrophy adaptations between low- vs. high-load resistance training: a systematic review and meta-analysis. J Strength Cond Res. 2017;31(12):3508-3523. doi:10.1519/jsc.0000000000002200.
1Corresponding author: Giullio César Pereira Salustiano Mallen da Silva, Rio de Janeiro State University, Rio de Janeiro, Brazil. Address: São Francisco Xavier Street, 524, Pavilhão João Lira Filho, 9º andar, Bloco F, sala 9134/5, Maracanã, Rio de Janeiro, RJ, Brasil, CEP: 20550-900. E-mail: giulliocesar.gc@hotmail.com
Rio de Janeiro State University, Rio de Janeiro, Brazil. https://orcid.org/0009-0001-6637-9020. yanndebrito@yahoo.com.
2 Rio de Janeiro State University, Rio de Janeiro, Brazil. https://orcid.org/0000-0001-8701-8550. giulliocesar.gc@hotmail.com.
3 Rio de Janeiro State University, Rio de Janeiro, Brazil. https://orcid.org/0009-0000-7898-049X. alex.meirelesrj@gmail.com.
4 Rio de Janeiro State University, Rio de Janeiro, Brazil. https://orcid.org/0009-0006-3590-6875. diegamalin@gmail.com.
5 Federal Rural University of Rio de Janeiro, Rio de Janeiro, Brazil. https://orcid.org/0000-0003-0413-0497. ravini.sodre@outlook.com.
6 Federal Rural University of Rio de Janeiro, Rio de Janeiro, Brazil. https://orcid.org/0009-0006-3590-6875. anabiamcm@gmail.com
7 Rio de Janeiro State University, Rio de Janeiro, Brazil. https://orcid.org/0000-0003-4972-650X. dirceurng@gmail.com.
8 Rio de Janeiro State University, Rio de Janeiro, Brazil. https://orcid.org/0000-0002-3049-8773. rodrigogsvale@gmail.com