Concurrent Guillain-Barré syndrome and longitudinally extensive myelopathy secondary to SARS-CoV-2 infection. Case report
Maria Isabella Bonilla Arbeláez1, D’angelo Clavijo Salazar2, Juan Felipe Cruz López3, Daniela Duque Montoya4
Recibido para publicación: 22-02-2024. Versión corregida: 29-04-2024. Aprobado para publicación: 27-06-2024.
Modelo de citación:
Bonilla Arbeláez M.I., Clavijo Salazar D, Cruz López J.F., Duque Montoya D,. Concurrent Guillain-Barré syndrome and longitudinally extensive myelopathy secondary to SARS-CoV-2 infection. Case report. Arch Med (Manizales). 2024;24(2). https://doi.org/10.30554/archmed.24.2.5044.2024
Abstract
Introduction: Severe acute respiratory syndrome caused by the severe acute respiratory virus SARS-CoV-2 may have a wide range of neurological manifestations. Guillain-Barré syndrome is a post-infectious acute polyneuropathy characterized by symmetrical and ascending flaccid paralysis, and is described as a complication of SARS-CoV-2 infection and other pathogens. Inflammatory myelopathies associated with the virus have also been described, among which transverse myelitis is the most frequent. Outstanding the autoinflammatory characteristics of both entities, concurrent presentation is possible. Case description: A 23-year-old male presented with pain and ascending acute weakness syndrome in the lower limbs with impossibility of urination and defecation over a 4-day course. The diagnosis of Guillain Barrè was made by electromyography, and thoracolumbar magnetic resonance imaging was performed, with findings of longitudinally extensive inflammatory myelopathy. An antibody test for SARS-CoV-2 was performed on the cerebrospinal fluid with a positive IgG result, considering neurological compromise due to the virus. Management was performed using plasmapheresis and methylprednisolone pulses, with a favorable response and hospital discharge. Discussion: The compromise of SARS-CoV-2 in the central and peripheral nervous systems is well known. Pathologies such as Guillain-Barrè syndrome have been widely reported and studied as a consequence of SARS-CoV-2 infection, and a variety of reports of longitudinally extensive inflammatory myelopathy associated with the pathogen have been published; however, the concurrence between both pathologies has been scarcely reported. Conclusions: It is necessary to consider a wide variety of atypical and even confluent presentations caused by infectious agents such as SARS-CoV-2 to achieve timely diagnosis and management that reduces morbidity and mortality in patients.
Keywords: Myelitis, Guillain-Barré syndrome, SARS-CoV-2, COVID-19.
Síndrome de Guillain-Barré concurrente y mielopatía longitudinal extensa secundaria a infección por SARS-CoV-2. Reporte de un caso
Resumen
Introducción: El síndrome respiratorio agudo grave causado por el virus respiratorio agudo grave SARS-CoV-2 puede tener una amplia gama de manifestaciones neurológicas. El síndrome de Guillain-Barré es una polineuropatía aguda postinfecciosa caracterizada por parálisis flácida simétrica y ascendente, y se describe como una complicación de la infección por SARS-CoV-2 y otros patógenos. También se han descrito mielopatías inflamatorias asociadas al virus, entre las que la mielitis transversa es la más frecuente. Destacando las características autoinflamatorias de ambas entidades, es posible la presentación concurrente. Descripción del caso: Varón de 23 años que presenta dolor y síndrome de debilidad aguda ascendente en miembros inferiores con imposibilidad de micción y defecación de 4 días de evolución. El diagnóstico de Guillain Barrè se realizó mediante electromiografía, y se realizó una resonancia magnética toracolumbar, con hallazgos de mielopatía inflamatoria longitudinalmente extensa. Se realizó una prueba de anticuerpos para SARS-CoV-2 en el líquido cefalorraquídeo con un resultado positivo de IgG, considerando el compromiso neurológico debido al virus. Se realizó manejo con plasmaféresis y pulsos de metilprednisolona, con respuesta favorable y alta hospitalaria. Discusión: El compromiso del SARS-CoV-2 en los sistemas nerviosos central y periférico es bien conocido. Patologías como el síndrome de Guillain-Barrè han sido ampliamente reportadas y estudiadas como consecuencia de la infección por SARS-CoV-2, y se han publicado diversos reportes de mielopatía inflamatoria longitudinalmente extensa asociada al patógeno; sin embargo, la concurrencia entre ambas patologías ha sido escasamente reportada. Conclusiones: Es necesario considerar una amplia variedad de presentaciones atípicas e incluso confluentes causadas por agentes infecciosos como el SARS-CoV-2 para lograr un diagnóstico y manejo oportuno que reduzca la morbimortalidad de los pacientes.
Palabras clave: Mielitis, síndrome de Guillain-Barré, SARS-CoV-2, COVID-19.
Síndrome de Guillain-Barré concomitante e mielopatia longitudinal extensa secundária à infecção por SARS-CoV-2. Relatório de um caso
Resumo
Introdução: A síndrome respiratória aguda grave causada pelo vírus respiratório agudo grave SARS-CoV-2 pode apresentar uma ampla gama de manifestações neurológicas. A síndrome de Guillain-Barré é uma polineuropatia aguda pós-infecciosa caracterizada por paralisia flácida simétrica e ascendente e é descrita como uma complicação da infecção por SARS-CoV-2 e outros patógenos. Também foram descritas mielopatias inflamatórias associadas ao vírus, entre as quais a mielite transversa é a mais frequente. Devido às características autoinflamatórias de ambas as entidades, é possível uma apresentação simultânea. Descrição do caso: Um homem de 23 anos apresentou dor e síndrome de fraqueza aguda ascendente nos membros inferiores com impossibilidade de urinar e defecar em um período de 4 dias. O diagnóstico de Guillain Barrè foi feito por eletromiografia, e foi realizada uma ressonância magnética toracolombar, com achados de mielopatia inflamatória extensa longitudinalmente. Um teste de anticorpos para SARS-CoV-2 foi realizado no líquido cefalorraquidiano com um resultado IgG positivo, considerando o comprometimento neurológico devido ao vírus. O tratamento foi realizado com plasmaférese e pulsos de metilprednisolona, com uma resposta favorável e alta hospitalar. Discussão: O comprometimento do SARS-CoV-2 nos sistemas nervosos central e periférico é bem conhecido. Patologias como a síndrome de Guillain-Barrè foram amplamente relatadas e estudadas como consequência da infecção pelo SARS-CoV-2, e vários relatos de mielopatia inflamatória extensa longitudinalmente associada ao patógeno foram publicados; no entanto, a simultaneidade entre as duas patologias foi pouco relatada. Conclusões: É necessário considerar uma ampla variedade de apresentações atípicas e até mesmo confluentes causadas por agentes infecciosos como o SARS-CoV-2 para obter um diagnóstico e um tratamento oportunos que reduzam a morbidade e a mortalidade dos pacientes.
Palavras-chave: Mielite, síndrome de Guillain-Barré, SARS-CoV-2, COVID-19.
Introduction
COVID-19 is an acute respiratory infection caused by the SARS-CoV-2 virus, declared a pandemic in 2020. The initial clinical symptoms were respiratory, with a broad spectrum ranging from mild upper respiratory symptoms to severe complications such as pneumonia, acute respiratory distress syndrome or shock, and organ failure.
Subsequently, a wide range of neurological signs and symptoms, such as anosmia, headache, vertigo, and others, are as severe as cerebrovascular attacks, acute encephalitis, and autoinflammatory syndromes [1].
Guillain-Barré syndrome is an acute polyneuropathy characterized by symmetric and ascending flaccid paralysis, which has been described as a post-infectious complication of some pathogens, including SARS-CoV-2. Few cases of myelopathy associated with Sars-Cov-2 have been described, including some cases manifesting as transverse myelitis. [2,3].
A case of concurrent Guillain Barré syndrome and longitudinally extensive transverse myelopathy secondary to SARS-CoV-2 infection is presented.
Case description
A 23-year-old male professional miner presented with pain, acute symmetric ascending weakness syndrome, loss of muscle strength, and impossibility of urination and defecation.
On physical examination, bilateral upper limb muscle strength was 5/5, and bilateral lower limb muscle strength was 0/5, with generalized areflexia without sensory alteration. The patient was febrile (38.9 °C) with a negative antigen test result for COVID-19. He was diagnosed with Guillain-Barrè Syndrome Hughes 4 and EGRIS 3 and was transferred to the intensive care unit. Treatment was performed with plasmapheresis, human immunoglobulin G (0.4/kg/day), and methylprednisolone pulses.
Due to early vesical incontinence, magnetic resonance imaging of the thoracolumbar spine was performed, which showed an alteration in the intensity of the spinal cord observed from the T2 level to the conus medullaris, which initiates in the anterior horns and then generalizes throughout the circumference of the spinal cord with significant thickening. These findings were consistent with longitudinally extensive transverse inflammatory myelopathy (Figure 1, 2, and 3).
Electromyography (EMG) described lumbosacral sensory-motor polyradiculoneuropathy of the axonal type. A cerebrospinal fluid (CSF) study showed slightly decreased glucose levels, increased protein levels, and neutrophilic pleocytosis (Table1). These results suggest a probable viral compromise, and we performed a study test for SARS-CoV-2 with a positive IgG result in the CSF, indicating neurological compromise as a consequence of infection by the pathogen.

Figure 1. MIR Sequence STIR: alteration in the intensity of the spinal cord observed from the T2 level to the conus medullaris, that initiates in the anterior horns and then generalizes throughout the circumference of the spinal cord with significant thickening of it

Figure 2. Sequence T2
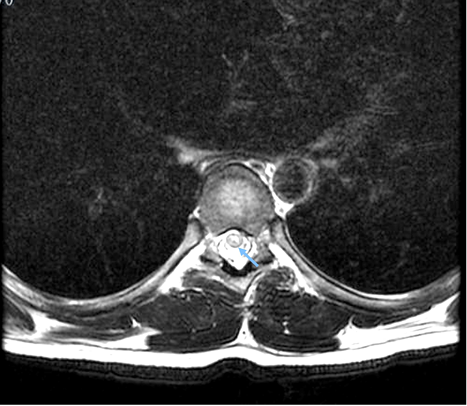
Figure 3. Sequence T2
The patient presented a favorable response to treatment, was transferred to a general hospital, and was discharged. The response to physical therapy was satisfactory, and at 3 months, the patient walked without support and had adequate sphincter control.
Table 1. CSF EXAMINATION
|
Color |
Colorless |
|
Appearance |
Clear |
|
Ph |
8.5 |
|
Density |
1020 |
|
Glucose |
47,9 mg/dl |
|
Protein |
88,2 mg/dl |
|
Leukocytes (WBC) |
70mm3 |
|
Neutrophils |
80% |
|
Lymphocytes |
20% |
|
Erythrocytes |
0 |
Discussion
Viruses have an extensive repertoire of routes to infect, evade, and damage the infinity of organisms for which they have tropism. In humans, there are viruses with high specificity for the central nervous system (CNS). However, viruses with respiratory tropism, such as influenza, respiratory syncytial virus, metapneumovirus, and coronavirus, frequently generate manifestations of the CNS, reaching there through mechanisms such as the hematogenous route or through peripheral and olfactory nerves [4], which are the pathways responsible for the arrival of SARS-CoV-2 in the central nervous system [5].
Since the beginning of the pandemic, the compromise that SARS-CoV-2 could cause in the nervous system has been described, from common symptoms such as fatigue or anosmia [1,3] to more serious and infrequent manifestations in the CNS and peripheral nervous system [6,7]. It has been proposed that these manifestations are a consequence of factors such as direct viral infection, which leads to cell death (autophagy, apoptosis, or pyroptosis) or neuroinflammation (overactivation of cytokines and cells of the immune system) [8].
This neuroinflammation, along with a dysregulated immune response, the production of autoantibodies, and antigenic mimicry, predisposes people to autoimmune presentations of viral diseases, including SARS-CoV-2 [9] and manifestations such as immune thrombocytopenic purpura, autoimmune hemolytic anemia, Kawasaki disease, Guillain Barrè syndrome, and transverse myelitis; the latter two are relevant in the present case [10].
Guillain-Barré syndrome (GBS) has been widely reported and studied as a consequence of SARS-CoV-2 infection, and approximately 70% of GBS cases have a history of viral infection [11].
The most recent meta-analyses and systematic reviews have shown variable data in the demographic and clinical presentation of patients with GBS secondary to COVID-19, which is a rare event in the pediatric population [12], with a prevalence of 0.15% (15 cases per 100,000 inhabitants) in adults [13]. Men were more affected than women (68.5% vs. 31.5%) and were not significantly associated with previous comorbidities presented by patients. Recently, vaccination against SARS-CoV-2 has been implicated in the generation of GBS, with a prevalence of 3.09 cases per million inhabitants [14,15].
Clinically, the vast majority of patients have symptoms of COVID-19 at the time of the neurological condition; however, asymptomatic cases have also been reported, as well as cases that present negative RT-PCR results for SARS-CoV-2 on admission, such as that observed in the present case [16].
The initial manifestations of GBS are sensory symptoms alone or in combination with paraparesis or tetraparesis, with a high prevalence of generalized areflexia. Ascending weakness progressing to flaccid tetraparesis and extension or persistence of sensory symptoms are the most common clinical course [14].
In a study of CSF, GBS classically presented an increase in proteins with a normal number of cells (albumin-cytological dissociation), which occurred between 56.6% and 71.2% of patients [13,14]. Our patient did not have this finding and presented with pleocytosis greater than 50 cells/μl, which suggests a different pathology; in this case, concomitant myelopathy.
In general, electrophysiological examination of patients with GBS shows polyradiculoneuropathy or sensorimotor polyneuropathy (as in the present case). EMG also reveals different patterns of GBS, among which acute inflammatory demyelinating polyneuropathy (AIDP) is the most common pattern in approximately 70-80% of cases [17].
Another pathology within the spectrum of autoimmune manifestations of SARS-CoV-2, which is closely related to the case presented, is acute myelopathy. These may be myelitis, defined as myelopathy due to inflammation within the spinal cord, demonstrated by CSF pleocytosis, an increased IgG index, and/or gadolinium enhancement. Symptom progression should have peaked within 2–21 days [18].
The most common form of myelitis is transverse myelitis, which presents with bilateral signs and a well-defined sensory level. Udinal extensive myelopathy is another variant of transverse myelitis, a spinal cord injury that extends to at least three segments of the spinal cord, and its association with SARS-CoV-2 is rarer [18]. This group of pathologies has a much lower incidence than GBS secondary to SARS-CoV-2 infection, mainly in case reports, case series, and systematic reviews [19–21].
Regarding the concurrence of pathologies, some cases of transverse myelitis and GBS have been reported after COVID-19 infection or vaccination [22,23]. However, while performing a non-systematic review of the literature on the concurrence between GBS and longitudinally extensive myelopathy secondary to SARS-CoV-2 infection, only a single case was found with this set of conditions in an 11-year-old female patient [24], which is possibly the first case reported in an adult population.
Conclusions
Neurological compromise associated with SARS-CoV-2 infection is highly relevant owing to its significant morbidity and mortality. In case acute weakness is present in the socio-demographic context of the current pandemic, it is necessary to be aware of the wide variety of atypical presentations, and even confluent, related to SARS-CoV-2 infection to achieve timely diagnosis and management that reduces morbidity and mortality in patients who suffer from them. The coexistence of Guillain-Barré syndrome and infectious myelopathy is infrequent, and its clinical suspicion is based on adequate anamnesis and clinical neurological examination.
References
1. Liu K, Pan M, Xiao Z, Xu X. Neurological manifestations of the coronavirus (SARS-CoV-2) pandemic 2019–2020. J Neurol Neurosurg Psychiatry. 2020;91:669–70.
2. Sheikh AB, Chourasia PK, Javed N, Chourasia MK, Suriya SS, Upadhyay S, et al. Association of Guillain-Barre syndrome with COVID-19 infection: An updated systematic review. J Neuroimmunol. 2021;355:577577.
3. Ahmad SA, Salih KH, Ahmed SF, Kakamad FH, Salh AM, Hassan MN, et al. Post COVID-19 transverse myelitis; a case report with review of literature. Ann Med Surg (Lond). 2021;69:102749.
4. Bohmwald K, Gálvez NMS, Ríos M, Kalergis AM. Neurologic Alterations Due to Respiratory Virus Infections. Front Cell Neurosci. 2018;12:386.
5. Meinhardt J, Radke J, Dittmayer C, Franz J, Thomas C, Mothes R, et al. Olfactory transmucosal SARS-CoV-2 invasion as a port of central nervous system entry in individuals with COVID-19. Nat Neurosci. 2021;24:168–75.
6. Maury A, Lyoubi A, Peiffer-Smadja N, de Broucker T, Meppiel E. Neurological manifestations associated with SARS-CoV-2 and other coronaviruses: A narrative review for clinicians. Rev Neurol (Paris). 2021;177:51–64.
7. Solomon T. Neurological infection with SARS-CoV-2 — the story so far. Nat Rev Neurol. 2021;17:65–6.
8. Keyhanian K, Umeton RP, Mohit B, Davoudi V, Hajighasemi F, Ghasemi M. SARS-CoV-2 and nervous system: From pathogenesis to clinical manifestation. J Neuroimmunol. 2021;350:577436.
9. Halpert G, Shoenfeld Y. SARS-CoV-2, the autoimmune virus. Autoimmun Rev. 2020;19:102695.
10. Yazdanpanah N, Rezaei N. Autoimmune complications of COVID-19. J Med Virol. 2022;94:54–62.
11. Wakerley BR, Yuki N. Infectious and noninfectious triggers in Guillain–Barré syndrome. Expert Review of Clinical Immunology. 2013;9:627–39.
12. Panda PK, Sharawat IK, Panda P, Natarajan V, Bhakat R, Dawman L. Neurological Complications of SARS-CoV-2 Infection in Children: A Systematic Review and Meta-Analysis. Journal of Tropical Pediatrics. 2021;67:fmaa070.
13. Palaiodimou L, Stefanou M, Katsanos AH, Fragkou PC, Papadopoulou M, Moschovos C, et al. Prevalence, clinical characteristics and outcomes of Guillain−Barré syndrome spectrum associated with COVID-19: A systematic review and meta-analysis. Eur J Neurol. 2021;28:3517–29.
14. Abu-Rumeileh S, Abdelhak A, Foschi M, Tumani H, Otto M. Guillain–Barré syndrome spectrum associated with COVID-19: an up-to-date systematic review of 73 cases. J Neurol. 2021;268:1133–70.
15. Wang F, Wang D, Wang Y, Li C, Zheng Y, Guo Z, et al. Population-Based Incidence of Guillain-Barré Syndrome During Mass Immunization With Viral Vaccines: A Pooled Analysis. Front Immunol. 2022;13:782198.
16. Aladawi M, Elfil M, Abu-Esheh B, Abu Jazar D, Armouti A, Bayoumi A, et al. Guillain Barre Syndrome as a Complication of COVID-19: A Systematic Review. Can J Neurol Sci. 2022;49:38–48.
17. Leonhard SE, Mandarakas MR, Gondim FAA, Bateman K, Ferreira MLB, Cornblath DR, et al. Diagnosis and management of Guillain–Barré syndrome in ten steps. Nat Rev Neurol. 2019;15:671–83.
18. Artemiadis A, Liampas A, Hadjigeorgiou L, Zis P. Myelopathy associated with SARS-COV-2 infection. A systematic review. Neurological Research. 2021;43:633–41.
19. Mondal R, Deb S, Shome G, Ganguly U, Lahiri D, Benito-León J. COVID-19 and emerging spinal cord complications: A systematic review. Multiple Sclerosis and Related Disorders. 2021;51:102917.
20. Schulte EC, Hauer L, Kunz AB, Sellner J. Systematic review of cases of acute myelitis in individuals with COVID-19. Eur J Neurol. 2021;28:3230–44.
21. Lee G. Acute longitudinal extensive transverse myelitis secondary to asymptomatic SARS-CoV-2 infection. BMJ Case Rep. 2021;14:e244687.
22. Canavero I, Ravaglia S, Valentino F, Micieli G. Guillain Barrè syndrome and myelitis associated with SARS-CoV-2 infection. Neuroscience Letters. 2021;759:136040.
23. Alrubaye R, Bondugula V, Baleguli V, Chofor R. A possible Guillain-Barré syndrome/transverse myelitis overlap syndrome after recent COVID-19. BMJ Case Rep. 2022;15:e246967.
24. Khera D, Didel S, Panda S, Tiwari S, Singh K. Concurrent Longitudinally Extensive Transverse Myelitis and Guillain-Barré Syndrome in a Child Secondary to COVID-19 Infection: A Severe Neuroimmunologic Complication of COVID-19. Pediatric Infectious Disease Journal. 2021;40:e236–9.
1 Estudiante de Medicina, Universidad de Caldas. https://orcid.org/0000-0001-6223-7685. isabellabonilla.ar@gmail.com
2 Médico General Universidad de Caldas. https://orcid.org/0000-0002-4416-3894?lang=en.
3 Médico General Universidad de Caldas. https://orcid.org/0000-0003-2207-0782.
4 Neuróloga Universidad de La Sabana. https://orcid.org/0000-0003-2067-1322.
