Artículo de Investigación sobre COVID-19
Lessons from the COVID-19 pandemic: knowledge and preventive actions among a mexican population sample
Enrique Konstat-Korzenny1, Dan Morgenstern-Kaplan2,
Rodrigo Fonseca-Portilla3, Ariel Cohen-Welch4
Medical doctor. Facultad de Ciencias de la Salud, Universidad Anáhuac México, México City, México. ORCID: 0000-0002-1297-3112. E-mail: enriquekonstat@gmail.com. Corresponding autor.
2 Medical doctor. Facultad de Ciencias de la Salud, Universidad Anáhuac México, México City, México. ORCID: 0000-0002-9031-2256. E-mail: dan.morgenstern@anahuac.mx
3 Medical doctor. Facultad de Ciencias de la Salud, Universidad Anáhuac México, México City, México. ORCID: 0000-0001-7130-0340. E-mail: rodrigo.fonseca@anahuac.mx
4 Medical doctor. Facultad de Ciencias de la Salud, Universidad Anáhuac México, México City, México. ORCID: 0000-0002-9526-3596. E-mail: Ariel.cohen@anahuac.mx
1Archivos de Medicina (Manizales) Volumen 21 N° 1, Enero-Junio 2021, ISSN versión impresa 1657-320X, ISSN versión en línea 2339-3874, Konstat-Korzenny E, Morgenstern-Kaplan D, Fonseca-Portilla R, Cohen-Welch A.
Recibido para publicación: 17-08-2020 - Versión corregida: 02-10-2020 - Aprobado para publicación: 08-10-2020
Konstat-Korzenny E, Morgenstern-Kaplan D, Fonseca-Portilla R, Cohen-Welch A. Lessons from the COVID-19 Pandemic: Knowledge and Preventive Actions Among a Mexican Population Sample. Arch Med (Manizales). 2021; 21(1):247-256. https://doi.org/10.30554/archmed.21.1.3965.2021
Summary
Objective: to evaluate the knowledge of the general population about the COVID-19 pandemic, including the disease and the preventive measures to reduce spreading of the virus undertaken by participants. Materials and methods: a cross-sectional study on a Mexican population sample was conducted during the period of March 20th to March 27th in Mexico, via a computer-based survey. General knowledge about COVID-19 and the adherence to recommendations were evaluated. Results: a total of 2,577 participants completed the survey. The results revealed an overall proper knowledge about the disease, with 76.2% having the proper knowledge about the disease, which was significantly correlated with age (r=0.15, p<0.001), socioeconomic status (r=0.06, p<0.003) and maximum academic level achieved by the study subjects (r=0.12, p<0.001). Conclusions: overall, people have good knowledge of COVID-19 and know about the specific public health recommendations, but a large proportion of people do not strictly follow these recommendations.
Keywords: COVID-19; pandemics; health surveys; preventive medicine.
Lecciones de la pandemia de COVID-19: conocimiento y acciones preventivas de una muestra de población mexicana
Resumen
Objetivo: evaluar el conocimiento de la población general acerca de la pandemia de COVID-19, incluyendo datos sobre la enfermedad y las medidas preventivas para reducir la propagación del virus. Materiales y métodos: se realizó un estudio transversal en una muestra de la población mexicana durante el periodo del 20 al 27 de marzo del 2020 por medio de una encuesta electrónica. Se evaluó el conocimiento general sobre COVID-19 y el apego a las recomendaciones de salud pública Resultados: 2,577 participantes completaron la encuesta. Los resultados muestran un adecuado conocimiento sobre la enfermedad en la población general (76.2% de la muestra), el cual está levemente correlacionado con la edad (r=0.15, p<0.001), estado socioeconómico (r=0.06, p<0.003) y grado académico (r=0.12, p<0.001). Conclusiones: en general, la población conoce la información acerca del COVID-19 y conoce las recomendaciones de salud pública, pero una gran proporción de la gente no sigue estrictamente estas recomendaciones.
Palabras Clave: COVID-19; pandemias; encuestas epidemiológicas; medicina preventiva.
Introduction
Coronaviruses are single-stranded, enveloped RNA viruses, whose name derive from their surface projections originating from the virion envelope, resembling a crown. [1,2] The virus can infect humans and animals, including bats, pigs, among others. Different viral strains have often gained the ability to infect humans, and in past decades, have been responsible for epidemics, such as the Severe Acute Respiratory Syndrome epidemic in 2003, and the Middle Eastern Respiratory Syndrome (MERS) in 2012 [3].
In December 2019, an emerging outbreak of atypical pneumonia was described in the province of Wuhan, China. Initial studies revealed as the etiological agent a novel coronavirus, later named SARS-CoV-2 due to its homology to a previously described bat coronavirus. [4,5]China, was caused by a novel betacoronavirus, the 2019 novel coronavirus (2019-nCoV The clinical entity was coined COVID-19 (Coronavirus Disease 2019). The virus initially spread to geographically close countries, including South Korea, Japan and Iran, thereafter to most of Europe, and eventually to the remaining countries of the globe within the next weeks, [6] urging the World Health Organization to classify the disease as a pandemic.
Regarding the virus origin, taxonomic studies were able to identify its close similitude to another bat coronavirus, which may have mutated to infect an intermediate host, an animal known as pangolin, which then further mutated again to infect humans [5,7,8].
The virus is mainly transmitted through respiratory droplets when people shedding the virus cough, sneeze or talk, and particles come in contact with mucous membranes. The virus can also remain viable on surfaces and infect a person through indirect contact. Evidence shows that infected but asymptomatic patients transmit the virus, as well as transmission through aerosol and airborne particles [9-13].
At the time of publication of this article, case reports and case series have been published and numerous clinical trials are being conducted to evaluate the efficacy of therapies for COVID-19 patients. Trials include the use of antiviral medications such as ritonavir-lopinavir and remdesivir, antibiotics such as teicoplanin, as well as azithromycin combinations with hydroxychloroquine. [14–19] Even though some of these studies provide interesting and promising findings, as of now, there is no sufficient and statistically significant evidence for health authorities and expert panels to recommend a definite treatment regimen for COVID-19 patients. The most effective way to halt the pandemic will be the development of a vaccine, which as of now, many protocols are still in Phase 3 studies. [20,21] However, that specific topic is beyond the scope of this work.
As the disease began to spread, governments started implementing measures to reduce the transmissibility and infection rate of the virus, which included strict travel restrictions and social distancing measures. It is worth mentioning that at that time there was far less information about the disease than what it is known presently. Since the initial development of the disease, citizens have been able to monitor and track different governments’ reactions and approaches to COVID-19, mainly through internet-based news platforms and social media. Digital platforms have proven their efficacy of spreading important and vital information in times of emergency but have also demonstrated their capacity to spread misinformation and unsupported facts and recommendations, causing panic and increased awareness by populations.
Particularly in Mexico, the government began its preventive measures by suspending schools and closing public recreational areas and businesses. They also began implementing information campaigns and encouraged physical and social distancing. The decisive government announcement for people to self-quarantine came on March 28th 2020, and the pandemic was finally declared a national emergency on March 30th 2020. By that time, various sectors of the population had already implemented the recommendations published by other countries and the World Health Organization (WHO), which included quarantining, working from home, avoiding public spaces and preventive hygiene measures.
The aim of the present study is to determine the level of COVID-19 knowledge, along with the degree of misinformation and panic-based decision-making present in the Mexican population across various population sectors. It is important to note that the questionnaire was applied quite early in the pandemic, and much of the information available both to the medical community and the general public was not available at the time.
Materials and methods
A cross-sectional study was performed on a Mexican population sample during the period of March 20th to March 27th in Mexico City and other states, via a computer-based survey that was directly administered to participants or self-taken online. Participants were recruited via virtual snowball sampling. Participants included male and female Mexican citizens over the age of 18, with Spanish as their native language. Exclusion criteria included non-native Spanish speakers and incomplete survey responses. Before starting the survey, participants agreed to take part in the research, and gave permission to use their answers in the statistical analysis for the present study. Names of the participants were not asked, as to allow for confidentiality. Only age, sex, salary, and level of maximal studies were asked.
The computer-based Spanish-written questionnaire (Table 1) was composed of four main sections: Section A, included general information and consent; Section B analyzed socioeconomic characteristics, Section C examined current COVID-19 preventive measures and social repercussions, finally Section D collected data of the knowledge about the disease itself.
Table 1. Complete survey about COVID-19 knowledge (Sections C, D)
|
Preventive measures against COVID-19 |
N |
% |
|
|
Daily hand-washing events before the pandemic |
1 |
91 |
3.5% |
|
2-3 |
815 |
31.6% |
|
|
4-5 |
906 |
35.2% |
|
|
6 or more |
765 |
29.7% |
|
|
Daily hand-washing events currently |
1 |
18 |
0.7% |
|
2-3 |
127 |
4.9% |
|
|
4-5 |
536 |
20.8% |
|
|
6 or more |
1896 |
73.6% |
|
|
Have you changed the way you greet people to a non-contact method? |
Yes |
2454 |
95.2% |
|
No |
123 |
4.8% |
|
|
Do you currently go outside to public places? |
Yes |
291 |
11.3% |
|
No |
2286 |
88.7% |
|
|
Do you currently visit family members? |
Yes |
913 |
35.4% |
|
No |
1664 |
64.6% |
|
|
Do you carry out a strict quarantine without going out anywhere? |
Yes |
385 |
14.9% |
|
No |
554 |
21.5% |
|
|
Only exceptionally |
1638 |
63.6% |
|
|
Do you know anyone who has been infected with COVID-19? |
Yes |
484 |
18.8% |
|
No |
2086 |
80.9% |
|
|
Have you cancelled any trips in this period? |
Yes |
1519 |
58.9% |
|
No |
1058 |
41.1% |
|
|
Have you traveled in this period? |
Yes |
502 |
19.5% |
|
No |
2075 |
80.5% |
|
|
Have you or your family suffered economic repercussions due to this pandemic? |
Yes |
1572 |
61.0% |
|
No |
1005 |
39.0% |
|
|
Have you done any panic-shopping? |
Yes |
371 |
14.4% |
|
No |
2206 |
85.6% |
|
|
Have you recently bought Hydroxychloroquine? |
Yes |
46 |
1.8% |
|
No |
2531 |
98.2% |
|
|
Do you consider that the Mexican government’s actions against the pandemic have been enough? |
Yes |
314 |
12.2% |
|
No |
1677 |
65.1% |
|
|
Undecided |
586 |
22.7% |
|
|
Do you know the government telephone number for assistance during this pandemic? |
Yes |
1775 |
68.9% |
|
No |
802 |
31.1% |
|
|
Knowledge of the virus |
N |
% |
|
|
What would you do if you presented symptoms of COVID 19? |
Go to the Hospital |
357 |
13.9% |
|
Stay Home |
375 |
14.6% |
|
|
Speak to a doctor |
1845 |
71.6% |
|
|
Where was this disease originated? |
China |
2539 |
98.5% |
|
Elsewhere |
38 |
1.5% |
|
|
Was this pandemic generated because someone ate a bat soup in another country? |
True |
1370 |
53.2% |
|
False |
1207 |
46.8% |
|
|
What are the ways to get infected from COVID-19? |
Respiratory Droplets |
2128 |
82.6% |
|
Sexual |
6 |
0.2% |
|
|
Trough the Skin |
248 |
9.6% |
|
|
Contact with Animals |
195 |
7.6% |
|
|
What organ system does the disease affect? |
Respiratory System |
2413 |
93.6% |
|
Nervous System |
7 |
0.3% |
|
|
Gastrointestinal Tract |
6 |
0.2% |
|
|
Immune System |
151 |
5.9% |
|
|
Is there an approved treatment for this disease? |
Yes |
168 |
6.5% |
|
No |
2409 |
93.5% |
|
Source: questionnaire asked to the evaluated sample.
Monthly wages were asked in local currency (Mexican peso) and further converted to US dollars based on the exchange rate of March 20th, 2020 (1 mxn = 0.0412 usd). The salary intervals in the survey are based on Mexican peso equivalents according to local minimum, average, and above average wages in the country. By government’s decree as of January 1st, 2020, the minimum monthly wage in Mexico is 3,690 mxn (152 usd) [22].
Data was collected with Google Forms (computer-based online survey software) and statistical analysis was performed in Microsoft Excel (Microsoft, 2020) and SPSS version 21.0 (IBM). Categorical variables were reported as frequencies and percentages. The Kolmogorov-Smirnov test was used to determine the distribution of numeric variables. Data were normally distributed; thus, correlation analysis was performed with the Pearson correlation coefficient and difference between numeric variables were analyzed with a paired samples T-test. Statistical significance was achieved with a p <0.05.
Results
Demographic Characteristics
A total of 2,634 participants completed the survey, 57 were excluded from the analysis due to incomplete or invalid responses. Of the total 2,577 analyzed responses, a slight majority were women, with a wide distribution in age groups and socioeconomic status, and most participants completed at least high school. Complete demographic data of the sample is expanded in Table 2.
Table 2. Demographic characteristics of the evaluated sample. (Questionnaire Sections A, B)
|
Demographic Characteristics |
N |
% |
|
|
Sex |
Male |
942 |
36.6% |
|
Female |
1635 |
63.4% |
|
|
Age in years |
<20 |
143 |
5.5% |
|
20-35 |
1029 |
39.9% |
|
|
36-59 |
1063 |
41.2% |
|
|
>60 |
342 |
13.3% |
|
|
Monthly salary (US Dollars) |
< $ 206 |
542 |
21.0% |
|
$207-$618 |
693 |
26.9% |
|
|
$619-$1,236 |
549 |
21.3% |
|
|
>$1,237 |
791 |
30.7% |
|
|
Finished High School |
No |
534 |
20.7% |
|
Yes |
2043 |
79.3% |
|
Source: questionnaire asked to the evaluated sample.
COVID-19 preventive measures, knowledge about COVID-19, social repercussions, and correlation analysis
Section C compiled data about the preventive and hygiene measures to reduce infections. Most participants of the study already knew and had adopted the measures collected in the survey, which were the current recommendations of the Mexican government at that time. Regarding hand hygiene, before the pandemic started, only 65% of the sample reported washing their hands 4 or more times daily, after the pandemic started, it increased to 94.2%, which was statistically significant (t=-48.2, p<0.001).
Social repercussions of the disease and the preventive measures were also analyzed in the survey, with 61% of the sample participants reporting economic repercussions, 60% reported cancellation of business and/or pleasure trips, 15% of the sample reported panic shopping in grocery stores and nearly 2% (n = 46) bought hydroxychloroquine or chloroquine as prophylaxis for COVID-19. Other results of this section are provided in Figure 1
. 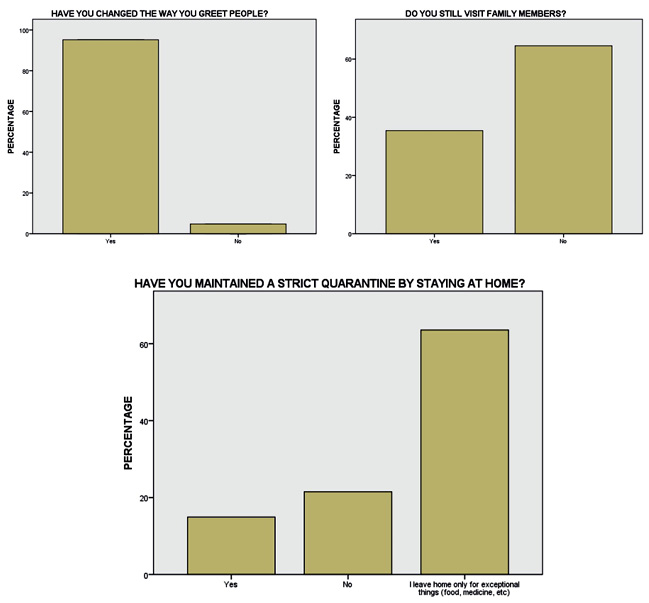
Figure 1. Adherence to recommendations from the Mexican Health Ministry during the period studied in the pandemic
Source: Questionnaire asked to the evaluated sample.
Section D asked several general knowledge questions about COVID-19 itself. Overall, 1,964 subjects (76.2%) had adequate general knowledge about the disease. The results had significant correlation with age (r=0.15, p<0.001), academic level (r=0.12, p<0.001) and socioeconomic status (r=0.06, p<0.003). Sources of information about the pandemic are portrayed in Figure 2.
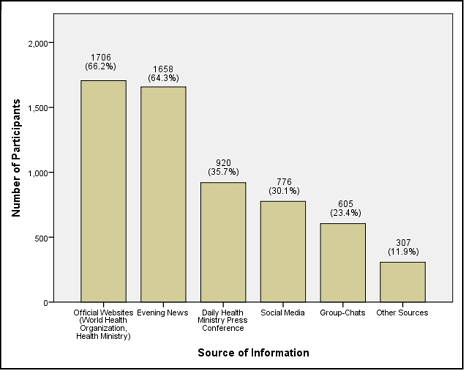
Figure 2. Reported sources of information about the COVID-19 pandemic
Source: Questionnaire asked to the evaluated sample.
Discussion
Due to their magnitude, pandemics require substantial effort not only from health professionals, but also cooperation from the general population. Disease awareness and appropriate preventive measures are important factors to mitigate the spread of the disease. In order to guarantee public participation, efficient information propagation is essential, which nowadays, is mainly accomplished through digital platforms. Mass communication platforms have allowed governments and health officials to make information readily available efficiently, but at the same time an opportunity for the spread of misinformation.
Through this survey, the level of knowledge and awareness of COVID-19 were rapidly and efficiently assessed before it was deemed a national emergency by the Mexican federal government and only a couple weeks after the WHO declared the disease a pandemic. Within the sample, there was a wide distribution of socioeconomic and educational status to determine the level of awareness about certain basic characteristics of the disease.
Most people are aware and participate in effective preventive measures encouraged by health personnel early in the pandemic. Social distancing and basic hygiene measures, like hand washing, were recognized by most people as important and necessary measures against the spread of disease.
The public is also properly informed about the mechanism of transmission and clinical symptoms of the disease. However, despite constant emphasis by health officials on criteria for visiting hospitals and/or emergency departments, a significant proportion of participants (13.9%) would visit these facilities even with mild symptoms. Health officials have made readily available platforms for citizens to describe symptoms and be advised on the appropriate course of action. Nonetheless, a significant proportion of the studied population (31.1%) are not aware of these tools made available to them, despite participants mentioning that their primary sources of information are official websites and broadcast television news.
These parameters used together, may be an indirect indicator of the effectiveness of information distribution by governments and health organizations. Differences can be identified, especially when analyzing the widespread recognition and acceptance by residents concerning preventive health measures, but more inconsistent awareness regarding government provided tools and resources. These differences in areas of knowledge can also be attributed to the other sources of information, in particular, social media and group chats. Through these platforms, sharing information between social groups may help propagate consciousness of some areas of concern, while displacing others regarded as less important.
Despite communication effectiveness by health officials, there is still a substantial area of opportunity for the spread of misinformation and false claims. This is especially true within social media platforms, where false or incomplete information can be generated and rapidly spread and shared throughout the world. This became evident and worrisome, for example, when it was identified that 2% of the studied population acquired hydroxychloroquine or chloroquine as a form of COVID-19 prophylaxis. At the time of preparation of this work, neither drug was recommended by health officials as effective evidenced-based treatment against COVID-19. Various research studies were being conducted at the time, but no official conclusions or recommendations had been made. Despite this, information was taken out of context and falsely spread that these medications were curative treatment for the disease, prompting citizens to acquire the drugs, possibly causing shortages of this drug used by other patients with rheumatologic conditions.
There is a generalized misconception about the origin of the virus, which may contribute to discriminatory practices against certain populations, especially the Asian community. These are merely some examples of how the speed and reach of communication platforms can spread high degrees of misinformation that lead to unfounded interventions by the public.
Finally, it is important to mention that a majority (65%) of the studied population disapproves or deems insufficient the actions taken by the Mexican health officials regarding the pandemic. It is difficult to determine the best course of action when facing a pandemic, especially when taking into consideration the substantial differences in socioeconomic disparities and health access among countries. Approach to pandemics will always be influenced by political, social, and economic determinants, and there cannot be a unifying course to be taken by all, although WHO promotes guidelines and suggestions to all member nations. This lack of approval and frustration may be secondary to the accessibility of information regarding measures taken by other countries worldwide, which now appear to have effectively controlled the spread of the virus, like South Korea and China. These measures may be more difficult to apply as they may not be economically viable in underdeveloped countries like Mexico, where the use of resources must be prioritized, causing nonconformity among citizens.
At present time, there is growing knowledge about the virus compared to when this survey was conducted, and approaches taken by certain countries have not been sufficient or have allowed for the spread of the virus. Official numbers on deaths and cases are most likely underdiagnosed, as there are not sufficient tests performed, especially in undeveloped nations, and there has been an obvious increase in overall deaths, most of which are not classified as COVID-19 cases, due to insufficient testing.
There are only a few recent articles that reflect the overall knowledge of the population about the current pandemic as it is an emergent topic. A similar study performed via online surveys in the United States and the United Kingdom, in March 2020, evaluated basic COVID-19 knowledge among the general population with similar results to our study, although many of their survey questions centered on different epidemiological aspects of the disease than the ones interrogated in this work. [23] Another article investigated COVID-19 knowledge by medical personnel, administrative personnel and medical students in a hospital setting in Mumbai, in April 2020, with overall proper knowledge about the disease by participants in their sample. [24] Roy and colleagues performed a similar online-based survey in April 2020 to 662 persons in India, with a similar socioeconomical distribution to the one presented in this study, and concluded that their studied population had “moderate” knowledge, and 98% of their sample would agree to quarantine if they presented fever and cough. [25] Kebede and colleagues published the results of a similar questionnaire assessing COVID-19 knowledge, published in May 2020, in Southwest Ethiopia. Their results showed overall adequate knowledge in their 247-person sample. [26] Honarvar and colleagues published in July 2020 a study assessing COVID-19 knowledge and risk perception in a sample population in Iran. They found inadequate overall knowledge about the disease, especially in the elderly, marginalized and lower educated people. [27] Siddiqui and colleagues found in a similar study in Saudi Arabia, published in August 2020, overall proper knowledge about COVID-19 and a statistically significant difference according to regions in their country [28].
The results portrayed in this study are concordant with the previous mentioned studies. Although the results obtained are promising and the sample demonstrated proper knowledge about the disease, official health authorities must still constantly address the population on COVID-19 preventive measures and reinforce basic knowledge to create awareness and prevent further infections and deaths.
Conclusions
The entire world is learning day by day about this novel infectious disease, and updates on scientific data will continue to emerge at fast rates. It is essential that health officials continue to inform their citizens on a regular basis about updates or changes in action plans against the disease to reduce the impact it will have on its population. Furthermore, the use of computer-based surveys are tools that can provide large amounts of information in an efficient and timely manner. Here, it allowed to identify population perceptions and knowledge about SARS-CoV-2. It is important to consider these types of tools in further studies, having in mind the limitations that they may imply.
With the results of this study, it has been demonstrated that people tend to be adequately informed about health issues and preventive measures during a pandemic outbreak, although there is still much more to be done. Overall, people are affected on a personal, social, and economic level by the novel virus, but have taken responsible and difficult decisions to contain the disease.
Study Limitations and Strengths
The sample, although large, was composed mostly of people with at least a complete basic education (high school), thus not fully representing most of the Mexican population, where the average studies are far below that. The limitations include a short time window to obtain our sample considering that people tend to be more informed as time passes, and official information campaigns are underway. Another limitation is that the information was obtained at the beginning of the pandemic, and there is substantially more information available to the public now. The snowball sampling method had to be used because of social distancing measures to avoid person to person contact during the pandemic. The strengths of this study are that a large sample of surveys was obtained and that it was done remotely, following the social distancing measures recommended by the WHO and other organizations. Furthermore, the results of this study can help other researchers in the field to improve the spread of preventive measures in these difficult times and might prove an example for future pandemics or sanitary emergencies. Also, this work provides solid information to evaluate alternatives to inform people about health-related issues.
Conflicts of interest: all authors declare no conflicts of interest for the present study.
Sources of funding: the authors provided all the necessary funds for this study.
Cited Literature
1. Tyrrell DA, Bynoe ML. Cultivation of viruses from a high proportion of patients with colds. Lancet. 1966; 1(7428):76–77. DOI: 10.1016/s0140-6736(66)92364-6
2. Velavan TP, Meyer CG. The COVID-19 epidemic. Trop Med Int Heal. 2020; 25(3):278–280. DOI: 10.1111/tmi.13383
3. Schoeman D, Fielding BC. Coronavirus envelope protein: Current knowledge. Virol J. 2019; 16(1):1–22. https://doi.org/10.1186/s12985-019-1182-0
4. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020; 395(10223):497–506. https://doi.org/10.1016/S0140-6736(20)30183-5
5. Zhou P, Yang XL, Wang XG, Hu B, Zhang L, Zhang W, et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature. ٢٠٢٠; 579(7798):270–273. http://dx.doi.org/10.1038/s41586-020-2012-7
6. Battegay M, Kuehl R, Tschudin-Sutter S, Hirsch HH, Widmer AF, Neher RA. 2019-novel Coronavirus (2019-nCoV): estimating the case fatality rate - a word of caution. Swiss Med Wkly. 2020; 150:1-3. DOI: 10.4414/smw.2020.20203
7. Zhang T, Wu Q, Zhang Z. Probable Pangolin Origin of SARS-CoV-2 Associated with the COVID-19 Outbreak. Curr Biol. 2020; 30(7) 1346–1351. https://doi.org/10.1016/j.cub.2020.03.022
8. Yuen KS, Ye ZW, Fung SY, Chan CP, Jin DY. SARS-CoV-2 and COVID-19: The most important research questions. Cell Biosci. 2020; 10(1):1–5. https://doi.org/10.1186/s13578-020-00404-4
9. Bai Y, Yao L, Wei T, Tian F, Jin DY, Chen L, et al. Presumed Asymptomatic Carrier Transmission of COVID-19. JAMA. 2020; 323(14):1406-1407. DOI: 10.1001/jama.2020.2565
10. Ong SWX, Tan YK, Chia PY, Lee TH, Ng OT, Wong MSY, et al. Air, Surface Environmental, and Personal Protective Equipment Contamination by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) from a Symptomatic Patient. JAMA. 2020; 323(16):1610-1612. DOI: 10.1001/jama.2020.3227
11. Rothe C, Schunk M, Sothmann P, Bretzel G, Froeschl G, Wallrauch C, et al. Transmission of 2019-NCOV infection from an asymptomatic contact in Germany. N Engl J Med. 2020; 382(10):970–971. DOI: 10.1056/NEJMc2001468
12. Anderson EL, Turnham P, Griffin JR, Clarke CC. Consideration of the Aerosol Transmission for COVID-19 and Public Health. Risk Anal. 2020; 40(5):902-907. DOI: 10.1111/risa.13500
13. Klompas M, Baker MA, Rhee C. Airborne Transmission of SARS-CoV-2: Theoretical Considerations and Available Evidence. JAMA. 2020; 324(5):441-442. DOI:10.1001/jama.2020.12458
14. Cao B, Wang Y, Wen D, Liu W, Wang J, Fan G, et al. A Trial of Lopinavir–Ritonavir in Adults Hospitalized with Severe Covid-19. N Engl J Med. 2020; 382:1787–1799. DOI: 10.1056/NEJMoa2001282
15. Wang M, Cao R, Zhang L, Yang X, Liu J, Xu M, et al. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Res. 2020; 30(3):269–271. https://doi.org/10.1038/s41422-020-0282-0
16. Dong L, Hu S, Gao J. Discovering drugs to treat coronavirus disease 2019 (COVID-19). Drug Discov Ther. 2020; 14(1):58–60. DOI: 10.5582/ddt.2020.01012
17. Colson P, Rolain JM, Raoult D. Chloroquine for the 2019 novel coronavirus SARS-CoV-2. Int J Antimicrob Agents. 2020; 55(3):10–11. DOI: 10.1016/j.ijantimicag.2020.105923
18. Baron SA, Devaux C, Colson P, Raoult D, Rolain JM. Teicoplanin: an alternative drug for the treatment of COVID-19? Int J Antimicrob Agents. 2020; 55(4): 1-2. https://doi.org/10.1016/j.ijantimicag.2020.105944
19. Gautret P, Lagier JC, Parola P, Hoang VT, Meddeb L, Mailhe M, et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: results of an open-label non-randomized clinical trial. Int J Antimicrob Agents. 2020; 56(1):1-2. https://doi.org/10.1016/j.ijantimicag.2020.105949
20. Folegatti PM, Ewer KJ, Aley PK, Angus B, Becker S, Belij-Rammerstorfer S et al. Safety and immunogenicity of the ChAdOx1 nCoV-19 vaccine against SARS-CoV-2: a preliminary report of a phase 1/2, single-blind, randomised controlled trial. Lancet. 2020; 396(10249):467-478. DOI: 10.1016/S0140-6736(20)31604-4.
21. Amanat F, Krammer F. SARS-CoV-2 Vaccines: Status Report. Immunity. 2020; 52(4):583-589. https://doi.org/10.1016/j.immuni.2020.03.007
22. Comisión Nacional de los Salarios Mínimos (México), Secretaría de Trabajo y Previsión Social. Salarios Mínimos 2020. Ciudad de México: Comisión Nacional de los Salarios Mínimos (México), Secretaría de Trabajo y Previsión Social; 2020.
23. Geldsetzer P. Knowledge and Perceptions of COVID-19 Among the General Public in the United States and the United Kingdom: A Cross-sectional Online Survey. Ann Intern Med. 2020; 173(3):157-160. DOI: 10.7326/M20-0912
24. Modi PD, Nair G, Uppe A, Modi J, Tuppekar B, Gharpure AS, et al. COVID-19 Awareness Among Healthcare Students and Professionals in Mumbai Metropolitan Region: A Questionnaire-Based Survey. Cureus. 2020; 12(4):1-18. DOI: 10.7759/cureus.7514
25. Roy D, Tripathy S, Kar SK, Sharma N, Verma SK, Kaushal V. Study of knowledge, attitude, anxiety & perceived mental healthcare need in Indian population during COVID-19 pandemic. Asian J Psychiatr. 2020; 51:1-7. https://doi.org/10.1016/j.ajp.2020.102083
26. Kebede Y, Yitayih Y, Birhanu Z, Mekonen S, Ambelu A. Knowledge, perceptions and preventive practices towards COVID-19 early in the outbreak among Jimma university medical center visitors, Southwest Ethiopia. PLoS One. 2020; 15(5):1-15. DOI: 10.1371/journal.pone.0233744
27. Honarvar B, Lankarani KB, Kharmandar A, Shaygani M, Zahedroozgar M, Rahmanian-Haghighi MR, et al. Knowledge, attitudes, risk perceptions, and practices of adults toward COVID-19: a population and field-based study from Iran. Int J Public Health. 2020; 65(6):731-739. DOI: 10.1007/s00038-020-01406-2
28. Siddiqui AA, Alshammary F, Amin J, Rathore HA, Hassan I, Ilyas M, et al. Knowledge and practice regarding prevention of COVID-19 among the Saudi Arabian population. Work. 2020; 66(4):767-775. DOI: 10.3233/WOR-203223
