Artículo de Investigación
Gestational syphilis in the low amazon mesoregion, Brazil, 2008 - 2018
Randerson-José de Araujo-Sousa1, Adriana-Vanessa Ribeiro-Mafra2,
Nádia-Vicência do Nascimento-Martins3, Luanna-Samara Ribeiro-Mafra4
1 Medical Student at the State University of Pará, Santarém, Brazil. ORCID: 0000-0003-3723-8955. E-mail: rajoarso@gmail.com
2 Medical Student at the State University of Pará, Santarém, Brazil. ORCID: 0000-0001-6014-7715. E-mail: mafra.dry@gmail.com
3 PhD in Science from the Nursing School of the University of São Paulo and Professor at the State University of Pará. ORCID: 0000-0002-8166-644X. E-mail: nadia.martins@uepa.br
4 Graduated in English from the Federal University of Western Pará, Santarém, Brazil. ORCID: 0000-0002-8032-7286. E-mail: luanna.mafra@outloock.com
Archivos de Medicina (Manizales) Volumen 21 N° 1, Enero-Junio 2021, ISSN versión impresa 1657-320X, ISSN versión en línea 2339-3874, de Araujo-Sousa RJ, Ribeiro-Mafra AV, do Nascimento-Martins NV, Ribeiro-Mafra LS.
Recibido para publicación: 01-05-2020 - Versión corregida: 11-08-2020 - Aprobado para publicación: 22-08-202
0
de Araujo-Sousa RJ, Ribeiro-Mafra AV, do Nascimento-Martins NV, Ribeiro-Mafra LS. Gestational syphilis in the low amazon mesoregion, Brazil, 2008 – 2018. Arch Med (Manizales). 2021; 21(1):67-76. https://doi.org/10.30554/archmed.21.1.3783.2021
Summary
Objective: to trace the epidemiological profile of gestational syphilis reported cases in the Low Amazon mesoregion in the period between 2008 and 2018. Materials and Methods: the study was epidemiological, observational, descriptive, retrospective, cross-sectional, and carried out by a quantitative approach. The variables were sociodemographic and epidemiological, and data was available by the Ministry of Health in line with the Department of Surveillance, Prevention, and Control of Sexually Transmitted Infections and Viral Hepatitis. The collected data were tabulated and processed with the aid of Microsoft Excel® 2010 and Action 3.7. Results: when characterizing the epidemiological profile, 949 cases were observed, which did not present normality; an average of 86.3 notifications per year; a median of 81; and a standard deviation of 47.6. The year 2017 stood out with 22.3% of notifications and the average age group was 24 years old. The race/color “brown” predominated with 87.6% and 42.7% did not have completed elementary school. The clinical classification that presented the highest records was “Primary Syphilis” with 49% and gestational age was “Third Trimester” with 50.3% of cases. The most adopted treatment regimen was Penicillin with 82.1%. There were ignored variables in the notification. Conclusion: given the results, it is clear that gestational syphilis is a public health problem in health care for women. Thus, this study can be used as a basis for public agencies to direct projects aimed at prevention and awareness about the consequences generated by the disease.
Keywords: public health; pregnant women; epidemiology.
Sífilis gestacional en mesorregión del bajo amazonas, Brasil, 2008 – 2018
Resumen
Objetivo: describir el perfil epidemiológico de los casos notificados de sífilis gestacional en la región del Bajo Amazonas de 2008 a 2018. Materiales y métodos: el estudio fue epidemiológico, observacional, descriptivo, transversal, con enfoque cuantitativo. Las variables eran sociodemográficas y epidemiológicas, y los datos fueron facilitados por el Ministerio de Salud de conformidad con el Departamento de Vigilancia, Prevención y Control de las Infecciones de Transmisión Sexual y las Hepatitis Virales. Los datos recogidos fueron tabulados y procesados con la ayuda de Microsoft Excel® 2010 y Action 3.7. Resultados: en la caracterización del perfil epidemiológico se observaron un total de 949 casos que no mostró normalidad, un promedio de 86,3 notificaciones por año, una mediana de 81 y una desviación estándar de 47,6. El año 2017 se destacó, con un 22,3% de las notificaciones. El promedio de edad era de 24 años. La raza/color “Marrón” predominaba con el 87,6% y el 42,7% no había completado la escuela primaria. La clasificación clínica con mayor número de registros fue “Sífilis primaria” con el 49% y la edad gestacional fue el “Tercer trimestre” con el 50,3% de los casos. El esquema de tratamiento más adoptado fue la penicilina con un 82,1%. Hubo variables ignoradas en la notificación. Conclusión: dado esto, está claro que la sífilis gestacional es un problema de salud pública en la atención de la salud de las mujeres. Por lo tanto, este estudio puede usarse como base para que las agencias públicas dirijan proyectos dirigidos a la prevención y la conciencia de las consecuencias generadas por la enfermedad.
Palabras clave: salud pública; mujeres embarazadas; epidemiología.
Introduction
Historically, syphilis was noted as a disease in France in the 15th century. Infected Spanish individuals spread this disease during the period of confrontation between France and Spain, due to the struggle for possession of Naples, causing the first epidemic of syphilis and, from that episode, it became known as french disease [1].
Syphilis is an infection caused by the bacterium Treponema pallidum, which can affect the entire body since it has multiple clinical manifestations [2]. It is sexually transmitted and it can present lesions or skin ulcerations, being a disease that develops slowly with alternations of symptomatic and asymptomatic periods. This disease is subdivided from the clinical manifestations into primary, secondary and tertiary syphilis [3].
This infection can be mainly acquired through sexual transmission but it can occur congenitally, when the mother vertically transmits to the child through the transplacental route. In this context, although the pregnant mother transmits the disease to her child, the case is not considered gestational syphilis, but congenital. Besides, this infection is extremely harmful to the life of the fetus, especially if the pregnant woman is not treated early, which can result in damage to fetal formation, abortion and death [4,5].
In the last 10 years, there has been an increase in the number of syphilis cases in Brazil, which may have occurred due to the better functioning of the surveillance system and greater access to rapid tests, since the Department of Surveillance, Prevention and Control of STDs, AIDS and Viral Hepatitis started to distribute almost six times the number of rapid tests [6].
On the other hand, many pregnant women with syphilis do not receive adequate treatment or any treatment, causing serious damage to the fetus, so the earlier the diagnosis and treatment of syphilis occur in pregnant women the lower the risk of vertical transmission and undesirable outcomes to the conceptus [7]. However, for this to happen, professionals need to be trained to understand the clinical evidence of syphilis, know and use laboratory tests and satisfactorily recognize the responses to treatment [8].
From this perspective, it is essential that as well as pregnant women their sexual partners are treated concurrently to avoid the high risk of reinfection, after all, Brazil adopts a partner with untreated infection as one of its criteria for defining syphilis cases [9]. Thus, even with countless difficulties, actions aimed at promoting health and tackling this type of infection have expanded access to health services for the Brazilian population through the Family Health Strategy (FHS) [10].
Regarding the North Region, in 2017 Pará was the state with the highest registered number of cases of gestational syphilis, being the first the state of Amazonas, according to the Epidemiological Bulletin of the Health Surveillance Secretariat of the Ministry of Health released in 2018 [11]. Thus, controlling this infection is a challenge for epidemiological surveillance services, in this sense, this study aimed to outline the epidemiological profile of the reported cases of gestational syphilis in the lower Amazon mesoregion, in the period between 2008 and 2018.
Materials and methods
Type of study:
The study was an epidemiological, observational, descriptive, retrospective, and cross-sectional study lead by a quantitative approach.
Research scenario:
The survey data correspond to the Low Amazon mesoregion (Figure 1) [12], which comprises a territory of 340,448.60 km² and is located in Brazil, northwest of the state of Pará. It consists of 14 municipalities, to be mentioned: Almeirim, Alenquer, Belterra, Curuá, Faro, Juruti, Monte Alegre, Óbidos, Oriximiná, Placa, Porto de Mós, Prainha, Santarém and Terra Santa [13]. The 14 municipalities were listed using the criterion of a greater number of inhabitants. After that, the first five municipalities were selected: “Santarém, Oriximiná, Monte Alegre, Alenquer and Óbidos”, according to the last census provided by the Brazilian Institute of Geography and Statistics [14].
Figure 1. Map Low Amazon Mesoregion of State of Pará, Brazil
Source: governo do estado do Pará (2019). Created by FAPESPA (2017) [12].
Sample size, selection of participants, and data source:
The study sample comprises the number of notified cases of gestational syphilis, made publicly available in the database of gestational syphilis of the Ministry of Health according to the Department of Surveillance, Prevention, and Control of Sexually Transmitted Infections (STI, HIV/AIDS) and Viral Hepatitis, from the Health Surveillance Secretariat. The notification forms, resulting from the prenatal consultations that are carried out throughout the Brazilian territory, feed this public access database.
For the study, all cases notified in the five municipalities selected from 2008 to 2018 were included, defining a sample of 949 eligible cases, that is, of pregnant women who were diagnosed with syphilis in health centers during prenatal care. Therefore, no type of interview and / or questionnaires were applied to patients and data were extracted only from the national epidemiological surveillance platform.
Collection variables and procedures:
From the database used, there were extracted sociodemographic variables: age range, education, race or color; and epidemiological variables: total cases, clinical classification, gestational age, and treatment scheme, with all variables recorded in terms of absolute frequency.
It is noteworthy that using the database filtering option was possible to check the number of notifications of gestational syphilis, by selected municipality, year by year, in the period from 2008 to 2018.
Statistical analysis:
The data collected by municipality were tabulated on Microsoft Excel® 2010 and, subsequently, were processed using the Action 3.7 software, through which estimated percentage was assigned to categorical variables and, for numerical variables, verification of data normality by the Shapiro - Wilk test with 5% significance level, and estimates of mean, median and standard deviation. Thus, reducing possible analysis bias, such as duplicate information. Finally, for the presentation of the results, graphs and tables were elaborated. No notified data was deleted and the ignored data was described.
Ethical aspects:
As this is data collected on a publicly accessible basis, the methodology did not pose a risk to the human person. Therefore, the research did not require the approval of an ethics and investigation committee.
Results
In the period from 2008 to 2018, 949 patients were analyzed when considering all the municipalities selected to compose the sample. The records correspond to the female gender, aged over ten years, and who were notified on the epidemiological surveillance platform of the Ministry of Health of Brazil as infected with syphilis during the gestational period (Table 1).
Table 1: Distribution of data reported by year in each municipality selected to constitute the sample of the low amazon mesoregion, Brazil
Sample Municipalities |
||||||
Year |
Santarém |
Oriximiná |
Óbidos |
Alenquer |
Monte Alegre |
Total |
2008 |
6 |
6 |
9 |
3 |
3 |
27 |
2009 |
24 |
15 |
5 |
6 |
4 |
54 |
2010 |
27 |
8 |
9 |
3 |
10 |
57 |
2011 |
36 |
10 |
11 |
9 |
3 |
69 |
2012 |
34 |
22 |
10 |
13 |
2 |
81 |
2013 |
65 |
22 |
5 |
9 |
12 |
113 |
2014 |
67 |
16 |
5 |
6 |
3 |
97 |
2015 |
43 |
9 |
5 |
7 |
5 |
69 |
2016 |
46 |
12 |
14 |
4 |
9 |
85 |
2017 |
140 |
26 |
18 |
18 |
10 |
212 |
2018 |
52 |
9 |
10 |
4 |
10 |
85 |
TOTAL |
540 |
155 |
101 |
82 |
71 |
949 |
Source: Ministry of Health/Department of Surveillance, Prevention, and Control of Sexually Transmitted Infections (STIs, HIV/AIDS) and Viral Hepatitis, from the Department of Health Surveillance (2019).
When analyzing the distribution of notifications by year, according to Table 1, this did not show normality in the data (p-value = 0.0131 <0.05), as well as showing an average of 86.3 notifications per year, a median of 81 and a standard deviation of 47.6, that is, with sample heterogeneity. The year of 2017 stood out, with 22.3% of notifications, followed by 2013 with 11.9% of total cases.
Regarding the age group, the data showed a normal distribution (p-value = 0.1297> 0.05) and the graphic analysis confirms this behavior given the decrease on both sides and the lower trend of extreme values (Figure 2). The age group that concentrated most records was 20 to 29 years old, with 52.6%, and subsequently, the age group 15 to 19 years old presented 29.1% of the total cases. In addition, the average age of notifications was approximately 24 years old, featuring a sample of young women. In this variable, there were no ignored cases.
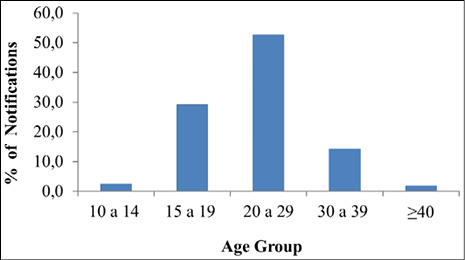
Figure 2. Percentage of notifications by age group from 2008 to 2018, in the Lower Amazon Mesoregion, Brazil
Source: Ministry of Health/Department of Surveillance, Prevention, and Control of Sexually Transmitted Infections (STIs, HIV/AIDS) and Viral Hepatitis, from the Department of Health Surveillance (2019).
As for the race/color of the notified patients, only 930 cases were registered on the platform that is, about 2% of the total notifications for this variable is not included in the database. In this sense, in percentage terms, in the period from 2008 to 2018, the race/color “Brown” predominated among the patients with 87.6%, followed by “White” with 5.8%, “Black” with 5.3%, “Yellow” with 0.8%, and “Indigenous” with 0.3%. Finally, there were 0.2% of notifications that ignored this variable.
Regarding education, there were 17.3% of ignored records, which in absolute terms, represents 164 patients who did not have their education level added to the platform during the analysis period. However, of the total number of notifications, 42.7% of pregnant women with syphilis did not have completed elementary school, while 1.2% had completed higher education (Figure 3).
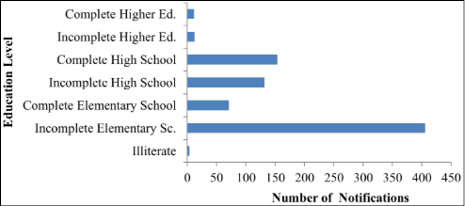
Figure 3. Absolute number of notifications of gestational syphilis according to the level of education in the period from 2008 to 2018 in the Lower Amazon Mesoregion, Brazil
Source: Ministry of Health/Department of Surveillance, Prevention and Control of Sexually Transmitted Infections (STIs, HIV/AIDS) and Viral Hepatitis, from the Department of Health Surveillance (2019).
Analysing the clinical classification of the notified patients, this variable was the one with the most ignored records, approximately 23.9% of cases, which is equivalent to 227 patients. However, when considering pregnant and infected women who had their classification recorded, the lowest concentration was in “Secondary Syphilis” with 7.6%, and “Primary Syphilis” was the classification that presented the highest records with 49% of diagnosed patients (Figure 4).
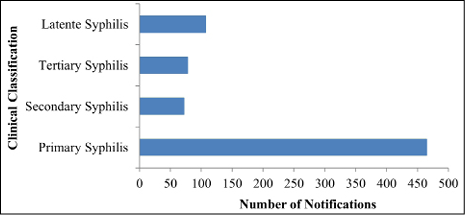
Figure 4. Absolute number of notifications of gestational syphilis according to the clinical classification from 2008 to 2018 in the Lower Amazon Mesoregion, Brazil
Source: Ministry of Health/Department of Surveillance, Prevention and Control of Sexually Transmitted Infections (STIs, HIV / AIDS) and Viral Hepatitis, from the Department of Health Surveillance (2019).
The gestational age at which the infection was detected was also a variable with ignored data and although it had a smaller number compared to those who also had this behavior, this variable presented 3.6%, which represents 34 patients without this information. At the same time, the “Third Trimester” was the age at which more women were diagnosed, equivalent to 50.3%, followed by the “Second Trimester” with 32.6% and, finally, the “First Trimester” with 13, 6% of reported cases.
As for the treatment scheme, the registrations started from the year 2014 and extended until 2017, so, for the remaining years, no information was obtained in the database. In this sense, there were 463 records for this variable: 82.1% corresponded to the scheme that used Penicillin; 5.6% represented another scheme that was not identified on the platform, in 5.4% of cases no scheme was carried out and 6.9% represented the ignored records.
Discussion
Based on the results, the profile of reported cases of gestational syphilis in the Low Amazon mesoregion is characterized. In this perspective, national references on the theme were sought for the better foundation of results. Thus, it was noticeable that the greatest number of cases of gestational syphilis occurred in women under the age of 30 years, following the results described in the research by Padovani [15], Dantas [16], Soares [17], Marques [18], and Lafetá [19]. Furthermore, this trend of results follows the national one presented in the 2018 epidemiological bulletin, released by the Ministry of Health, in which it is described that young people between 15 and 30 years old are the most infected with syphilis during pregnancy [20].
It is possible to infer that this finding may be related to the early sexual initiation of adolescents, as well as to the choice for the low frequency of using or not using condoms during sexual intercourse. This is highlighted in studies by Oliverira [21] and -Costa [22] in which adolescents and young people stated that they use infrequently or do not use condoms when they have sexual intercourse, pointing to trust in their partners as a justification.
Regarding race/color variable, in one hand, the results corroborate the study by Cavalcante [23], carried out in the northern region of Brazil, in which most of the pregnant women declared themselves to be brown in color. On the other hand, they diverge from findings in a study by Cardoso [24], carried out in the southern region of the country, in which the majority declared themselves to be white. At the same time, research carried out in other Brazilian regions, also presented similar results to this study, such as the findings of Dantas [16] and Soares [17].
It is worth pointing out that when referring to the issue of color, the study by Santos [25], which addresses socioeconomic aspects related to health, places a pertinent position when showing that there is a high prevalence that, in general, groups people considered “non-white” have an unsatisfactory quality of health. In this, sense, this reality notably dues to unequal access to health care, directly related to color.
Concerning the levels of education, the predominance of cases in women who have only incomplete elementary education followed the findings of Cardoso [24], Magalhães [26], Dantas [16], and Nonato [27], in which low education was a factor of great expressiveness among pregnant women infected with syphilis. According to Germano [28], low education is linked to less absorption of educational information about prevention, in addition to the association of this aspect with the non-return for the control of the disease, that is, the non-continuity of the treatment.
In relation to clinical classification, the data of this research corroborated those of Oliveira [21] and Dantas [16], in which there was a greater predominance of diagnosis of gestational syphilis in the primary phase. On the other hand, the results of this study disagreed with the findings by Marques [18] that presented most prevalence in tertiary phase of gestational syphilis.
Considering gestational age, the results showed a higher frequency of gestational syphilis during the third trimester of pregnancy, differing from the study by Oliveira [21], in which there was a greater prevalence of cases of gestational syphilis in the second trimester of gestation. For this research, it is worth emphasizing the importance of assessing the findings for this variable, since there is a high percentage of risk of vertical transmission of syphilis, especially in the last trimester of pregnancy.
In this context, cases of syphilis in the third trimester require attention, because, according to Febrasgo [4], there is an increase in the permeability of the placental barrier in proportion to the evolution of gestational age, which may result in congenital syphilis. Besides, another important point to be discussed and related to these data is the late start of prenatal care, especially for young people and adolescents, groups with a higher number of cases of gestational syphilis that may occur due to frequent cases of pregnancy unplanned in this period of development [29,21].
As for the treatment scheme, the results found by Oliveira [21] were similar to those reported in this study, since penicillin was also the drug of choice to treat pregnant women affected by syphilis. In respective order and decreasing frequency of use, it was used Penicillin G benzathine 7,200,000UI, Penicillin G benzathine 2,400,000UI, and Penicillin G benzathine 4,800,000UI, depending on the stage of the disease.
It is noteworthy that there was a shortage of benzathine penicillin in 2015, due to the lack of raw materials for the manufacture of first choice medicine for the treatment of syphilis, but which had been reported by municipalities and states since 2014 [30]. These shortages may also have been the result of the fact that this medication is a low-cost product that generates an unsatisfactory profitable return for manufacturers or even a market competition [31,18].
In addition, it is important to emphasize that the adoption of treatment with benzathine penicillin is very beneficial since it is included in the National List of Essential Medicines (RENAME). From this insertion, this medicine is also part of the strategic component of pharmaceutical assistance in primary care, so pregnant women may obtain it in Basic Health Units (UBS) in Brazil or through the low-cost Popular Pharmacy Program [3].
Conclusion
From the given data, it is clear that cases of gestational syphilis occur mainly in adolescents and young people under the age of thirty, brown in color, whose predominant level of education is incomplete primary education. Most syphilis infections are diagnosed when the disease is in the primary phase and the third trimester of gestation is the most frequent gestational age in this study, with penicillin as the first choice for the pregnant woman’s treatment regimen. In addition, it is important to highlight the frequency of ignored data in several variables, which can hinder the construction of an epidemiological profile for cases of gestational syphilis in the studied region.
Thus, this research can be used as a basis for public health agencies to have a general perception about the syphilis cases in pregnant women in the low Amazon mesoregion, to direct projects focusing on the dissemination of information about prevention and raising awareness about the consequences generated by the disease. In addition, this study is instigating for the development of new research with this theme in the interior of the Brazilian Amazon, since the approach of this theme in scientific works is still quite restricted in this region.
However, this study was limited by conditions related to socio-cultural aspects and the lack of public policies. The latter being reflected in the absence of health professionals in remote and rural locations; the insufficient training of working professionals; the precariousness or the absence of physical and technical structure, such as computer and internet access, which can lead to numerous underreporting in addition to restricting the possibility of data collection regarding other variables.
Therefore, this scenario prevented a recognition of the real health condition of pregnant women living in the mesoregion of the lower Amazon although it does not make the research less relevant given the need to evaluate the scenario of gestational syphilis, especially in this part of the Brazilian Amazon.
Author’s contribution
The entire design process of this study, to mention: collection, processing, data analysis, construction of the introduction topics, methodology, results, discussion, conclusion, as well as the critical analysis of this study, were carried out by all authors, who collaborated expressively and in the same way throughout the development.
Acknowledgments
The authors would like to thank the Ministry of Health of Brazil, which, in line with the Department of Surveillance, Prevention and Control of Sexually Transmitted Infections (STIs, HIV/AIDS) and Viral Hepatitis, of the Health Surveillance Secretariat, provide data on this topic, so that they are analysed and contextualized.
Conflicts of interest: none.
Financing sources: the authors are the suppliers.
Cited literature
1. Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de DST, Aids e Hepatites Virais. Sífilis: Estratégias para Diagnóstico no Brasil. Brasília: Ministério da Saúde, Coordenação de Doenças Sexualmente Transmissíveis e Aids. 2010. 100 p. Série TELELAB; 2010.
2. Costa CV, Santos IAB, Silva JM, Barcelos F, Guerra HS. Sífilis congênita: repercussões e desafios. Arq Catar de Med. 2017; 46(3):194-202.
3. Brasil. Sífilis 2018. Curitiba: Secretaria de Saúde do Estado do Paraná. Boletim Epidemiológico do Estado do Paraná; 2018.
4. Febrasgo. Sífilis. São Paulo: Federação Brasileira das Associações de Ginecologia e Obstetrícia; 2017.
5. World Health Organization (WHO). Who guideline on syphilis screening and treatment for pregnant women. Geneva: World Health Organization; 2017.
6. Brasil. Ministério da Saúde. Sífilis 2016. Brasilia: Secretaria de Vigilância em Saúde, 2016. Boletim Epidemiológico; 2016.
7. Nunes OS, Zara ALSA, Rocha DFNC, Marinho TA, Mandacarú PMP, Turchi MD. Sífilis gestacional e congênita e sua relação com a cobertura da Estratégia Saúde da Família, Goiás, 2007-2014: um estudo ecológico. Epidemiol Serv Saú. 2018; 27(4):1-10. DOI: 10.5123/S1679-49742018000400008
8. Maraschin M, Rocha A, Tonini NS, Souza EA, Caldeira S. Caracterização de indivíduos acometidos por sífilis adquirida e congênita em um município do oeste do Paraná. Rev Nurs. 2018; 21(243):2294-2298.
9. Lago EG. Current Perspectives on Prevention of Mother-to-Child Transmission of Syphilis. Cureus. 2016; 8(3):1-20. DOI: 0.7759/cureus.525
10. Arantes LJ, Shimizu HE, Merchán-Hamann E. Contribuições e desafios da estratégia saúde da Família na Atenção Primária à saúde no Brasil: revisão da literatura. Ciên & Saú Col. 2016; 21(5):1499-1509. DOI: 10.1590/1413-81232015215.19602015
11. Brasil. Ministério da Saúde. Sífilis 2017. Brasilia: Secretaria de Vigilância em Saúde, 2017. Boletim Epidemiológico; 2017.
12. Governo do Estado do Pará. Região de Integração do Baixo Amazonas. Pará: Secretaria de Estado de Desenvolvimento Agropecuário e da Pesca; 2019.
13. Ibge. Projeto Levantamento e Classificação do Uso da Terra no Estado do Pará. Rio de Janeiro: Instituto Brasileiro de Geografia e Estatística; 2013.
14. Ibge. População no último censo. Brasilia: Instituto Brasileiro de Geografia e Estatística; 2010.
15. Padovani C, Oliveira RR, Pelloso SM. Sífilis na gestação: associação das características maternas e perinatais em região do sul do Brasil. Rev Latino-Am Enferm. 2018; 26:1-10. DOI: 10.1590/1518-8345.2305.3019
16. Dantas LA, Jerônimo, SHNM, Teixeira, GA, Lopes, TRG, Cassiano, NA, Carvalho, JBL. Perfil epidemiológico de sífilis adquirida diagnosticada e notificada em hospital universitário materno infantil. Enferm glob. 2017; 16(46):217-226. http://dx.doi.org/10.6018/eglobal.16.2.229371
17. Soares BGMR, Marinho MAD, Linhares MI, Mota DS. Perfil das notificações de casos de sífilis gestacional e sífilis congênita. SANARE. 2017; 16(02):51-59. https://doi.org/10.36925/sanare.v16i2.1178
18. Marques JVS, Alves BM, Marques MVS, Arcanjo FPN, Parente CC, Vasconcelos RL. Perfil epidemiológico da sífilis gestacional: clínica e evolução de 2012 a 2017. SANARE. 2018; 17(02):13-20. https://doi.org/10.36925/sanare.v17i2.1257
19. Lafetá KRG, Martelli Júnior H, Silveira MF, Paranaí LMR. Sífilis materna e congênita, subnotificação e difícil controle. Rev Bras de Epide. 2016;19(1): 63-74. DOI: 10.1590/1980-5497201600010006
20. Brasil. Ministério da Saúde. Sífilis 2018. Brasilia: Secretaria de Vigilância em Saúde, 2018. Boletim Epidemiológico; 2018.
21. Oliveira RBB, Peixoto AMCL, Cardoso MD. Sífilis em gestantes adolescentes de Pernambuco. Adoles & Saúd. 2019; 16(2):47-55.
22. Costa COM, Santos BC, Souza KEP, Cruz NLA, Santana MC, Nascimento OC. HIV/AIDS e sífilis entre gestantes adolescentes e adultas jovens: fatores de exposição e risco dos atendimentos de um programa de DST/HIV/AIDS na rede pública de saúde/SUS, Bahia, Brasil. Rev Baian de Saúd Públi. 2011; 35(1):179-195.
23. Cavalcante NS, Lima HRR, Tabosa DF, Barbosa ESS, Costa NPS, Costa LM, et al. Syphilis in female sex workers: an epidemiological study of the highway system of the state of Pará, northern Brazil. Rev da Soc Bra de Med Trop. 2018; 52:1-5. DOI: 10.1590/0037-8682-0064-2018
24. Cardoso ARP, Araújo MAL, Cavalcante M, Frota MA, Melo SP. Análise dos casos de sífilis gestacional e congênita nos anos de 2008 a 2010 em Fortaleza, Ceará, Brasil. Ciên & Saú Col. 2018; 23(2):563-574.
https://doi.org/10.1590/1413-81232018232.01772016
25. Santos JAF. Desigualdade racial de saúde e contexto de classe no Brasil. DADOS – Rev de Ciên Soci. 2011; 54(1):5-40. http://dx.doi.org/10.1590/S0011-52582011000100001
26. Magalhães DMS, Kawaguchi IAL, Dias A, Calderon IMP. A sífilis na gestação e sua influência na morbimortalidade materno-infantil. Ciên Saú. 2011; 22(1):43-54.
27. Nonato SM, Melo APS, Guimarães MDC. Sífilis na gestação e fatores associados à sífilis congênita em Belo Horizonte-MG, 2010-2013. Epidemiol. Serv. Saúd. 2015; 24(4):681-694. DOI: 10.5123/S1679-49742015000400010
28. Germano FN, Da Silva TMG, Mendoza-Sassi R, Martínez AMB. Alta prevalência de usuários que não retornam ao Centro de Testagem e Aconselhamento (CTA) para o conhecimento do seu status sorológico - Rio Grande, RS, Brasil. Ciên & Saúd Colet. 2008; 13(3):1033-1040. https://doi.org/10.1590/S1413-81232008000300026
29. Alves EVG, Campos KFC, Fonseca TG, Araújo A. Estudo dos antecedentes perinatais de mães adolescentes em Buenópolis/Minas Gerais. R Enferm Cent O Min 2014; 3(4):1300-1309. DOI: https://doi.org/10.19175/recom.v0i0.771
30. Brasil. Ministério da Saúde. Nota Informativa Conjunta Nº 109/2015/GAB/SVS/MS, GAB/SCTIE/MS. Brasilia: Secretaria de Vigilância em Saúde; 2015.
31. Portal médico. Brasil enfrenta aumento da incidência de sífilis em gestantes e bebês. Brasília: Conselho Federal de Medicina (CFM); 2017.
