Research Article 

Compliance to treatment in diabetic patients from Bucaramanga, Colombia: a cross sectional study
Juan Manuel Ospina Díaz 1, Luz Jimena Martínez 2, Laura Victoria Ospina Ariza 3, Silvia Juliana Bueno 3, Héctor Hernando Gutiérrez 3, Paul Anthony Camacho López 4.
1 MD Magíster en Epidemiología. Profesor Titular Escuela de Medicina UPTC- Tunja, Boyacá; Grupo de investigación Biomédica y de Patología. Tunja, Colombia. ORCID: http://orcid.org/0000-0002-3476-2287. Correo e.: juan.ospina@uptc.edu.co
2 MD Nutricionista dietista. Docente Facultad de Ciencias de la Salud Universidad Autónoma de Bucaramanga UNAB., Grupo de Cardiología Preventiva. Bucaramanga, Colombia. Correo e.: lmartinez@unab.edu.co
3 MD Interno Universidad Autónoma de Bucaramanga UNAB. Grupo de Cardiología Preventiva, Bucaramanga, Colombia. ORCID: http://orcid.org/0000-0003-2659-222X. Correo e.: lospina280@unab.edu.co ; ORCID: http://orcid.org/0000-0002-7309-5173, Correo e.: sbueno192@unab.edu.co; ORCID: http://orcid.org/0000-0002-0124-6876, Correo e.: hgutierrez2014@unab.edu.co
4 MD Magíster en Epidemiología. Docente asociado Facultad de Ciencias de la Salud Universidad Autónoma de Bucaramanga UNAB. Grupo de Cardiología Preventiva. Bucaramanga, Colombia. ORCID: http://orcid.org/0000-0002-6233-9582. Correo e.: pcamacho@unab.edu.co.
Archivos de Medicina (Manizales), Volumen 19 N° 1, Enero-Junio 2019, ISSN versión impresa 1657-320X, ISSN versión en línea 2339-3874. Ospina Díaz J.M., Martínez L.J., Ospina Ariza L.V. Bueno S.J., Gutiérrez H.H., Camacho López P.A.
Recibido para publicación: 23-11-2018 - Versión corregida: 10-02-2019 - Aprobado para publicación: 11-03-2019
Ospina-Díaz JM, Martínez LJ, Ospina-Ariza LV, Bueno SJ, Gutiérrez HH, Camacho López PA. Compliance to treatment in diabetic patients from Bucaramanga, Colombia: a cross sectional study. Arch Med (Manizales) 2019; 19(1):23-1. DOI: https://doi.org/10.30554/archmed.19.1.2877.2019.
Summary
Objective: this study is aimed to evaluate knowledge about the disease, some behavioral habits and the level of compliance to pharmacological treatment, in a sample of diabetic patients, attending at hospital institution in the city of Bucaramanga (Colombia), during 2016. Diabetes mellitus is a chronic disease whose prevalence is increasing significantly in developing countries. Materials and Methods: cross sectional, descriptive study; a sample of 411 diabetic, aged over 35 years, who consulted at cardiovascular risk program, answered in the period between January and December 2016, a self-administered questionnaire that included the instruments IMEVID, Berbés and modified SMMS; Additionally, sociodemographic variables such as age, sex, stratum, education, were included. Results: 90% had a low socioeconomic status and 82.7% only reached primary studies or less. High Pharmacological adherence was observed in only 3.65%, medium adherence in 87.83% and low at 8.52%. Mean level of knowledge about diabetes was 13.32; Almost half (46.72%) scored below the average; Mean of glycosylated hemoglobin was 7.93%; 34.8% scored above this value. 18.7% have an inadequate lifestyle (IMEVID score <60). Low adherence found associated with: alcohol intake, IMEVID score <60, Ask more after eating, have a job and don’t use insulin. Conclusion: it is necessary to establish learning strategies and methodologies of motivation and training for diabetic patients, to improve quality of life and knowledge of the diabetes and, in this way, optimize the prognosis of the disease.
Keywords: diabetes mellitus, patient compliance, healthy lifestyle, patient medication knowledge.
Adherencia al tratamiento en pacientes diabéticos de Bucaramanga, Colombia: estudio de corte transversal
Resumen
Objetivo: el estudio se propone evaluar el conocimiento sobre la enfermedad, algunos hábitos de comportamiento y el nivel de cumplimiento con el tratamiento farmacológico en una muestra de pacientes diabéticos que asistieron a una institución hospitalaria en la ciudad de Bucaramanga (Colombia) durante el 2016. La diabetes mellitus es una enfermedad crónica, su prevalencia está aumentando significativamente en los países en desarrollo. Materiales y Métodos: estudio de corte transversal, descriptivo; una muestra de 411 diabéticos, mayores de 35 años, que consultaron al programa de riesgo cardiovascular, respondieron en el período comprendido entre enero a diciembre de 2016, un cuestionario autoadministrado que incluía los instrumentos IMEVID, Berbés y SMMS modificado; Adicionalmente, se incluyeron variables sociodemográficas como edad, sexo, estrato, educación. Resultados: el 90% tenía un estatus socioeconómico bajo y el 82.7% solo alcanzó estudios primarios o menos. Se observó una alta adherencia farmacológica en solo el 3,65%, una adherencia media en el 87,83% y una baja en el 8,52%. El nivel medio de conocimiento sobre la diabetes fue de 13.32; Casi la mitad (46.72%) puntuó por debajo del promedio; La media de hemoglobina glicosilada fue de 7.93%; El 34.8% puntuó por encima de este valor. El 18.7% tiene un estilo de vida inadecuado (puntuación IMEVID <60). Se encontró que la baja adherencia estaba asociada con: consumo de alcohol, puntaje IMEVID <60, pedir más después de comer, tener un trabajo y no usar insulina. Conclusión: es necesario establecer estrategias de aprendizaje y metodologías de motivación y entrenamiento a los pacientes diabéticos, para mejorar la calidad de vida y el conocimiento de la diabetes, y de esta manera, optimizar el pronóstico de la enfermedad.
Palabras clave: diabetes mellitus, cooperación del paciente, estilo de vida saludable, conocimiento de la medicación.
Introduction
Diabetes mellitus (DM) is a chronic disease whose pathophysiological substrate is characterized by the inability of the pancreas to synthesize or release insulin or, when the cells gradually lose the ability to incorporate and use insulin. Currently, DM has been recognized as a public health problem worldwide [1]. In 2015, it is estimated that, in the world, around 415 million suffer of this disease and 318 million have prediabetes, that is, they are at risk of developing microvascular complications, since global prevalence has almost doubled in the period 2014 - 2018 [2]. In high-income countries, DM implies very high costs of care, due to the occurrence of major cardiovascular diseases such as blindness, kidney failure and lower limb amputation, sequelae consistent with deficient control of DM. Maintaining blood levels of blood glucose, blood pressure and cholesterol close to normal can help delay or prevent the progression of DM [3].
In the perspective of the care and clinical control of the diabetic patient, efforts are focused on balancing serum glucose levels, for which drug-therapeutic interventions and changes in lifestyle habits are designed, especially in the diet, physical activity and self-care by the patient. The biggest obstacle in this perspective is given by the urgent need for the patient to accept and adopt a lifestyle, frequently extent unusual, because the magnitude of the restrictions that must be adopted to achieve stability [3]. This is reflected because around 50% of patients maintain blood sugar levels above the recommended limits [4].
With the aim of establishing the magnitude of events in which the patient follows the self-care instructions and complies with the indications of therapeutic prescription, various terms have been coined from the academy to identify this dimension. Thus, the terms adherence, attachment, compliance (in English, the most used are compliance and adherence) [5]. There are multiple definitions that aim to integrate this concept, adherence is defined as the event in which two conditions are positive: compliance in the taking of medications and persistence during the formulation time [6].
Another definition disseminated by the World Health Organization (WHO), considers adherence as “a continuum in which, each patient reaches a degree of self-behavior focused on the taking of medicines, monitoring a diet and acquisition of habits that configure a healthy lifestyle, in correspondence with the recommendations given by a health agent “, in this case, the definition goes beyond the concept of pharmacological adherence, because it also involves behavioral changes [7].
What really is considered an aspect of singular importance, in the case of the DM, is to be able to access indicators of adherence, through procedures that can be direct or indirect. In our environment, indirect methods are more common, given the ease of application of previously designed and validated questionnaires or questionnaires [8], of which in the case of DM, the most used is that of Morinsky-Green, which consists of four questions that inquire about whether the patient takes the medication, if he forgets to take it and if he suspends it when he feels good or bad, although this scale only quantifies the behaviors related with the fact of taking the medication [9].
Another important factor to consider, in order to study in depth the phenomenon of adherence, is related to the costs and the quality and duration of life in patients affected by DM, since the adequate control of the glycemia levels, depend principally of the cardiovascular integrity and, of certain particularly labile structures such as feet, peripheral nerves, eyes and kidneys [10]. The aim of this study was to evaluate the knowledge about the disease, behavioral habits and the level of compliance to pharmacological treatment, in diabetic patients attending a hospital institution in the city of Bucaramanga, during 2016.
Materials and methods
There was designed an observational, descriptive, cross sectional study. The target population was the community of patients diagnosed as DM, who attend to the cardiovascular prevention program at the Local Hospital of the North (HLN) located at the city of Bucaramanga (Colombia). The study was approved by the Institutional Ethics Committee of the HLN. All potential participants were duly informed of the study object and methodology and them expressed their consent to participate, in each moment, the researchers procured to respect confidentiality and privacy of the subjects.
Sample size was estimated from a reported prevalence of adherence to treatment of 34.1% [11], with type I error of 0.05, an acceptable margin of error of 5% and type II error of 20%, which yielded a sample size of 398 patients, selected from a target population of about 1200 diabetics enrolled in the cardiovascular risk program; finally, 411 people who met the eligibility criteria were linked; they answered a self-administered questionnaire in the period between January to December 2016. Sampling was carried out following a non-probabilistic sequential plan, as a result of which a total of 411 patients were interviewed. The inclusion criteria were taken into account: men and women over 35 years of age, with a confirmed diagnosis of DM, linked to the cardiovascular risk program of the Hospital del Norte de Bucaramanga. As exclusion criteria, the habitual consumption of steroids by any medical indication, pregnant women, terminal illness, severe prostration, iron deficiency anemia or manifest inability to answer the questionnaire was considered.
Sources of information were a survey that included sociodemographic variables (sex, age, occupation, socioeconomic stratum and type of affiliation to the Health System), clinical variables (time elapsed since the diagnosis of DM, glycemia values and glycosylated hemoglobin at the time of the last control). For the purposes of quantifying the degree of pharmacological adherence, lifestyle and knowledge about the disease, the following instruments were included: the modified 4-item Morinsky-Green questionnaire, the IMEVID questionnaire and the Berbés questionnaire.
The modified Morinsky-Green questionnaire is an instrument conformed of 4 questions, which ask about whether the patient takes the medication, if he forgets to take it and if he usually suspends it when he feels good or bad; This is a context, in addition to the therapeutic regimen, such as diet, physical activity and control of associated risk factors [12]. the Spanish version of this scale was validated by Val-Jiménez et al. [13].
The IMEVID questionnaire. The IMEVID (Instrument to Measure the lifestyle in Diabetics), helps the primary care physician to quantify the lifestyle of patients suffering DM, considering the following dimensions: nutrition, physical activity, tobacco consumption, alcohol intake, knowledge about diabetes, emotion management and therapeutic compliance. This questionnaire consists of 25 closed questions. Each item presents three response options with ratings of 0, 2 and 4, where 4 corresponds to the maximum desirable value in each response, for a total score of 0 to 100, with no odd values on the scale. moreover, this result allows patients to be classified into 3 groups: the first: ≤ 60, group 2: 60-78 and group 3, ≥ 80. allowing in this way, an adequate analysis of patients according to their score; the Spanish version of this scale was validated by López-Carmona et al. [14].
The Berbés questionnaire, is an instrument that allows assessing the degree of knowledge of the patients about their disease, expressed in the case of evaluation studies as mean ± standard deviation (SD). The instrument consists of 18 questions: 13 scored from -1 to 1 and 5 questions scored from -2 to 2; with which the score of the test can range between -23 and 23 points [13]; the Spanish version of this scale was validated by Andrés-Iglesias et al. [15]. Data were collected in the period between February and December 2016, through structured direct interview.
Statistical analysis. It was used the Epi-Info7™ program (OMS-CDC Atlanta, USA). Qualitative data are expressed as percentages and the quantitative data as mean and standard deviation according with the frequency distribution. Confidence limits were calculated at 95% (CI), using the Chi2 tests for qualitative variables and, in the case of small samples, the Fisher variant. Student’s t test for quantitative variables when the distributions were normal (Kolmogorov test with the Lilliefors corrections) and Mann-Whitney (Wilcoxon) for variables without normal distribution. The correlations were determined by the Pearson r or Spearman’s Rho according to whether or not they were parametric variables. The statistical significance was fixed at p <0.05. Bias control was achieved by sample size and diagnostic verification. The included confounding variables were the subject of stratified analysis.
Results
Characterizing the sample. Of 411 subjects, 76.6% (n = 315) were female; mean age was 62.25 years (SD = 11.7, range 35-93), no statistically significant differences were found in the mean age by sex (p = 0.17); 67.7% of male with stable partners, in contrast to 43.5% female (p = 0.0001). Only 1.95% of the subjects are jubilated, while 79.8% are unemployed. 90% belong to socioeconomic stratum 1-2, only 9.9% stratum 3-4. 82.7% barely reached complete primary education or less.96.3% are linked to the health system in the subsidized modality, while only 3.7% are as contributory.
The average value of fasting blood glucose was 162.42 mg / dL (SD = 78.02) with a statistically significant difference in benefit of female (159.27 ± 71.9 mg / dL) compared to men (172.75 ± 94.9 mg / dL).
The mean value of the glycosylated hemoglobin was 7.93% (SD = 2.13, range 5-16.5%); no statistically significant differences were found by sex. 59.65% (n = 241) of the patients registered fasting blood glucose above 126.0 mg / dL, which reflects inadequate management and control of diabetes. 34.8% (N = 143) registered percentages above 8%, which is interpreted as inadequate control of serum levels of glycemia, during at least the last three months.
There was a low degree of positive correlation between the values of fasting glycemia and the glycosylated hemoglobin, the Pearson correlation coefficient (R) was 0.58; the goodness of fit, expressed as R2= 0,34; p value (Prob >F) =0,0000 (Figure 1).
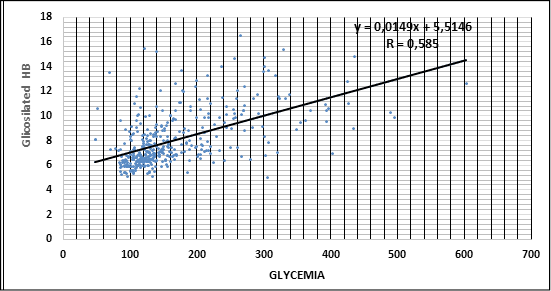
Figure 1. Correlation between Glycemia and Hemoglobin Glycosylated (HbA1C). Diabetic patients from Bucaramanga 2016. (Prob. > F= 0,0000). Source: Database. Own elaboration
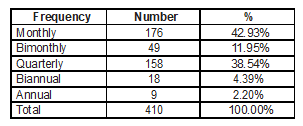
The mean time of permanence as diabetic patient was 6.95 years (SD = 6.46, range 0.1-45); no statistically significant differences were found by sex. 34.8% of patients (n = 140) are located above this average. Table 1 shows the frequency with which these patients attend to control meet.
Table 1. Frequency of the control meet. Diabetic patients from Bucaramanga, 2016.
Source: database. Own elaboration.
36.74% (n = 151) are insulin-dependent while the others consume other types of medications, mainly oral hypoglycemia agents. The most used insulin is the prolonged release one.
In measuring the lifestyle of diabetics, the starting suppose, is that when higher scores are in the IMEVID instrument, the levels of fasting blood glucose and glycosylated hemoglobin must be lower. The mean score of the IMEVID test was 69.73 (SD = 9.62, range 40-94); Table 2 shows the mean values of glycosylated hemoglobin and glycemia in relation to the score group reached in the IMEVID questionnaire. There were no statistically significant differences between the groups (p> 0.05).
Table 2. Mean values of Glycosylated Hemoglobin (HbA1C) and fasting blood glucose accord to IMEVID score. Diabetic patients from Bucaramanga, 2016.

Source: database. Own elaboration.
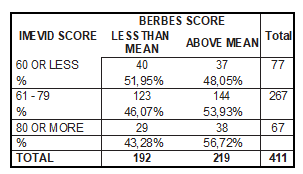
In the assessment of the degree of knowledge that patients have about the disease, the mean score was 13.32 (SD = 4.5, range 4 - 23). Almost half, that is, 46.72% (n = 192) of the subjects scored below the mean; Table 3 correlates the scores obtained in the IMEVID and Berbés tests by the patients included.
Table 3. Relationship between the scores in the test IMEVID and Berbés. Diabetic patients from Bucaramanga, 2016.
Source: database. Own elaboration.
Using the modified Morinsky-Green questionnaire, the degree of pharmacological adherence to the treatment of diabetes was estimated; it was found to be high in only 3.65% (n = 15) patients, medium in 87.83% (n = 361) and very low in 8.52% (n = 35).
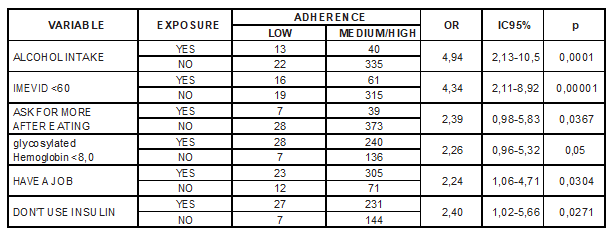
In an exploratory way, there were sought to establish some degree of causal association between the low level of pharmacological adherence with some factors present in the corresponding instruments. Table 4 shows the most significant correlations that were found.
Table 4. Assessing possible association between low pharmacological adherence to treatment and some possible risk factors. Diabetic patients from Bucaramanga 2016.
.
Source: database. Own elaboration.
Discussion
There is a worldwide consensus that the management of diabetic patients can’t be restricted to drug-therapy; The integral and rational management of the DM disease requires the adoption of a lifestyle that includes: an strict and balanced diet, regulated and constant physical activity, permanent control of body weight and abandonment of potentially harmful habits such as smoking and exaggerated consumption of alcoholic beverages [16].
Although the majority of patients registered a medium level of adherence to pharmacological treatment, it’s worrisome that this indicator is not optimal for most patients; It is convenient to review in detail the strategy and methodology of training and motivation, that should be included for the diabetic patient control program, which in essence should include the social and sociocultural aspects that have the most significance for the purpose of achieving a more committed attitude to self-care and rigor in aspects such as diet, physical activity and hygienic precautions [17].
There is some consensus, considering that the complications of diabetes can be significantly reduced if patients persist on maintaining adequate control of their glycemic figures, by combining therapeutic measures and self-care, particularly because intensive control of blood glucose by reducing the overall rate of microvascular complications by up to 25% [18].
It is also important to consider that a significant majority of the population included in the study has a very low grade of education, too a precarious socioeconomic status, then, they come from a segment of the population living in poverty, which is why it is very important the design and implementation of educational and training strategies that guarantee a high impact on the socio-cultural and economic aspects mentioned, which should undoubtedly be expressed in the significant changes in the style of life, quantifiable in the IMEVID instrument and also on the level of knowledge about diabetes, measurable through the Berbés instrument [19].
Several studies have shown that the level of knowledge about the disease significantly affects the quality of life and the degree of compliance of patients, since dissatisfaction results in demotivation and skepticism about achieving an appropriate level of well-being [20].
The glycosylated hemoglobin is emerging as a very reliable indicator of the degree of control, acceptance and adherence of the patient to pharmacological treatment and to the patterns of behavior and diet that turn out to be significantly beneficial for the management and control of their disease, since it allows to a certain extent predict microvascular lesions as well as the circulatory system in general. When comparing the levels of glycosylated hemoglobin with lifestyle, the level of knowledge about the disease, the time of evolution and the degree of acceptance and adherence, it is found that when the lifestyle is appropriate and patients have adequate knowledge of the disease is more likely to achieve metabolic and functional stability, expressed as glycosylated hemoglobin values less than 8% [19].
The low degree of economic status that was found in this study shows forward another disadvantage, constituted by the degree of food security of adults with diabetes, a concept that implies having access to a healthy diet. It has been seen that, in populations with high index of food insecurity, consumption of sugars and carbohydrates soars, while in communities that enjoy food security there is a better dietary balance [21].
Limitations of this study
Although this study offers a panoramic view of the problem that occurs with the adherence and knowledge of diabetic patients about their disease, it is important to consider that because it is a cross-sectional study, the results should be taken with caution, since it offers a perspective, but not It can be considered a conclusive result. In any case, these results invite to carry out analytical studies designed with greater rigor approach.
Conclusions
It is found in the group of diabetics treated in the Hospital del Norte de Bucaramanga, a very low socioeconomic and educational level that, coupled with pedagogic and strategic deficiencies in health education and lack of motivation aimed at adopting an appropriate lifestyle. the disease, lead to a very low percentage of high adherence to pharmacological treatment.
Conflict of interest: none
Funding sources: this project was financed with the resources of the “Grupo de Medicina Clínica y de Patología” and “Grupo de Cardiología Preventiva”, research collectives.
Cited literature
1. Organización Mundial de la Salud (OMS). Informe Mundial sobre la diabetes. Resumen de orien- tación. Ginebra: Organización Mundial de la Salud (OMS); 2016.
2. International Diabetes Federation. Atlas de la Diabetes de la FID. 6º ed. Bruselas: International Diabetes Federation; 2015.
3 Avalos MI, López C, Priego HR, Córdoba JA, Mo- rales MH. Barreras y perspectivas del personal de salud en el control de la diabetes mellitus en unidades médicas de la seguridad social en Ta- basco: un estudio cualitativo. Horizonte sanitario
2013; 12(3):111-118. DOI: https://doi.org/10.19136/
hs.a12n3.
4 Ibarra-Costilla E, Cerda R, Martínez L, Echeverry M, Calzado C, Villa S, et al. ¿Es el esquema de tratamiento un posible factor causal de estrés oxidativo en pacientes con Diabetes Mellitus Tipo 2? Resúmenes. Rev Invest Clin 2004; 56(6):817-818.
5 Libertad MA. Acerca del concepto de adheren- cia terapéutica. Rev Cub Salud Publica 2004;
30(4):0-0.
6 Nogués X, Sorli ML, Villar J. Instrumentos de me- dida de adherencia al tratamiento. An Med Interna
2007; 24(3):138-41.
7 Organización Mundial de la Salud. Adherencia a los tratamientos a largo plazo: Pruebas para la acción. Ginebra: Organización Panamericana de la Salud; 2004.
8 Ho PM, Bryson CL, Rumsfeld JS. Medication Adherence: Its Importance in cardiovascular outcomes. Circulation.2009; 119(1):3028-3035. DOI: 10.1161/CIRCULATIONAHA.108.768986.
9 Peralta ML, Carbajal-Pruneda P. Adherencia al tratamiento. Rev Cent Dermatol Pascua 2008;
17(3):84-8.
10 Pérez-Rodríguez A, Berenguer-Gouarnaluses M. Algunas consideraciones sobre la diabetes mellitus y su control en el nivel primario de salud. MEDISAN 2014; 19(3):375-390.
11 Fornos JA, Ferrer JC, García P, Huarte J, Molinero A, Mera R, et al. La diabetes en España desde la perspectiva de la farmacia comunitaria: conocimiento, cumplimiento y satisfacción con el tratamiento. Farmacéuticos Comunitarios
2016; 8(2):5-15. DOI:10.5672/FC.2173-9218.(2016/ Vol8).002.02.
12 López LA, Romero SL, Parra DI, Rojas LZ. Ad- herencia al tratamiento: concepto y medición. Hacia Promoc Salud 2016; 21(1):117-137. DOI:
10.17151/hpsal.2016.21.1.10.
13 Val Jiménez A, Amorós G, Martínez P, Fernández ML, León M. Estudio descriptivo del cumplimien- to del tratamiento farmacológico antihipertensi- vo y validación del test Morisky y Green. Aten Primaria 1992; 10:767-70.
14 López-Carmona JM, Rodríguez-Moctezuma JR, Ari- za-Andraca CR, Martínez-Bermúdez M. Estilo de vida y control metabólico en pacientes con dia- betes Mellitus tipo 2. Validación por constructo del IMEVID. Aten Primaria 2004; 33(1):20-27.
15 Andrés-Iglesias JC, Andrés-Rodríguez NF, Fornos- Pérez JA. Validación de un cuestionario de conocimientos sobre hipercolesterolemia en la farmacia comunitaria. Seguimiento Farmacotera- péutico 2005; 3(4):189-196.
16 Figueroa ME, Cruz JE, Ortiz AR, Lagunes AL, Ji- ménez J, Rodríguez JR. Estilo de vida y control metabólico en diabéticos del programa Diabe- tIMSS. Gac Méd Méx 2014; 150(1):29-34.
17 Brooks AD, Rihani RS, Derus CL. Pharmacist Membership in a Medical Group’s Diabetes Health Management Program. Am J Health- Syst Pharm 2007; 64(6):617-21. DOI:10.2146/ ajhp060095.
18 UK Prospective Diabetes Study Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with Type2 diabetes (UKPDS 33). Lancet 1998; 352:837-53.
19 Figueiredo IV, Moteiro C, Castel-Branco MM, Ca- ramona MM, Fernández-Llimos F. Seguimiento de pacientes con diabetes tipo 2 en una unidad de atención primaria de salud. Pharm Care Esp
2014; 16(2):39-48.
20 Andrés Rodríguez NF, Fornos Pérez JA, Andrés Iglesias JC. Valoración del conocimiento/cumpli- miento en un programa de seguimiento farma- coterapéutico en diabéticos tipo 2 en farmacia comunitaria: estudio aleatorizado. Pharm Care Esp 2007; 9(1):2-9.
21 González GJ, Martínez K, Betancourt B, Medina AK, Castillo AM, Monroy R. Seguridad alimentaria en el adulto mayor que vive con diabetes mellitus tipo 2 en León, Guanajuato. Rev jóvenes en la ciencia 2018; 2(1):104-107.
