Vaginal colonization and vulvovaginitis by Candida species in pregnant women from Northern of Colombia
Paola Suárez 1, Ana Belloz2, Martha Puelloz3, Gregorio Youngz4, Marlene Duranz5, Alicia Arechavala 6
1. MSc. Cartagena University. Mail Corresponding author: psuareza@unicartagena.edu.co
2. MD. Specialist. Cartagena University. amabet2001@hotmail.com
3. Professional. Cartagena University. mpuellohoyos@yahoo.com
4. Specialist. Cartagena University. greyoung@hotmail.com
5. PhD. Cartagena University. mduranl@unicartagena.edu.co
6. PhD. Mycology Unit, Hospital de Infecciosas Muñiz, Buenos Aires, Argentina. aliarecha@hotmail.com
Archivos de Medicina (Manizales), Volumen 18 N° 1, Enero-Junio 2018, ISSN versión impresa 1657-320X, ISSN versión en línea 2339-3874. Suárez P.; Bello A.; Puello M.; Young G.; Duran M.; Arechavala A.
Recibido para publicación: 10-06-2017 - Versión corregida: 12-03-2018 - Aprobado para publicación: 12-04-2018
Suárez P., Bello A., Puello M., Young G., Duran M., Arechavala A. Vaginal colonization and vulvovaginitis by Candida species in pregnant women from Northern of Colombia. Arch Med (Manizales) 2018; 18(1):51-9. DOI: https://doi.org/10.30554/archmed.18.1.2010.2018.
Summary
Objective: identify the vaginal colonizing Candida species and VVC species, predisposing factors and susceptibility against fluconazole in pregnant women attending gynecological outpatient of a maternal clinic in Cartagena (Colombia). Vulvovaginal candidiasis (VVC) is a common infection that affects a large proportion of women of childbearing age. It is estimated that about 75% of healthy women have had at least one episode of VVC in her life. Vaginal colonization by Candida spp. can vary from 10 to 17% and this is increased by 35% during pregnancy. The epidemiological behavior of Candida in VVC tends to be variable and this will depend on the level of vaginal estrogens, conditions of immunosuppression or chronicity of the process. Materials and Methods: the laboratory study included the direct examination of vaginal swabs, by fresh and differential staining of smears and cultures. The isolated species were identified by phenotypic tests and by multiplex PCR and CLSI M27-A3 microdilution method was used to evaluate susceptibility to fluconazole. Results: the frequent clinical diagnosis of bacterial vaginosis, did not correspond with the laboratory diagnosis in which predominated the intermediate biota. The results showed Candida albicans as the most common isolated species, followed by Candida tropicalis and Candida krusei. Candida colonization occurred in 71.4% and 28.6% of the population was diagnosed with vaginal candidiasis. All isolates were susceptible to fluconazole. Conclusion: The most common factors for colonization were related to clothing and for vaginal candidiasis to the use of vaginal lubricants.
Key Words: candida, candidiasis, vulvovaginal, pregnant women.
Vulvovaginitis y colonización vaginal por especies de Candida en gestantes del norte de Colombia
Resumen
Objetivo: identificar las especies colonizantes y asocidadas a CVV, factores predisponentes y sensibilidad a fluconazol en gestantes que asistieron a la consulta externa ginecológica de una clínica materna de Cartagena (Colombia). La candidiasis vulvovaginal (CVV) es una infección común que afecta una gran proporción de mujeres en edad fértil. Se estima que un 75% de las mujeres sanas han tenido al menos un episodio de CVV en su vida. La colonización vaginal por Candida spp. varía del 10 al 17% y esta alcanza un 35% durante el embarazo. El comportamiento epidemiológico del género Candida en la VVC es variable y dependerá del nivel de estrógenos de la vagina, inmunosupresión o cronicidad del proceso. Materiales y métodos: el estudio de laboratorio comprendió, examen directo de exudados vaginales, mediante fresco y tinciones diferenciales. Los aislamientos se identificaron por pruebas fenotípicas y PCR múltiple y se utilizó el método M27-A3 del CLSI por microdilución para la evaluación de la sensibilidad a fluconazol. Resultados: el diagnóstico médico frecuente de vaginosis bacteriana no correspondió con el de laboratorio en el que predominó la biota intermedia. Los resultados revelaron a Candida albicans como la especie más frecuente, seguida por Candida tropicalis y Candida krusei. La colonización por Candida fue del 71,4% y la candidiasis vaginal del 28,6%. Los aislamientos resultaron sensibles a fluconazol. Conclusión: los factores más frecuentes para colonización se relacionaron con la ropa y para candidiasis vaginal, con el uso de lubricantes vaginales.
Palabras clave: candida, candidiasis vulvovaginal, mujeres embarazadas.
Introduction
Vulvovaginal candidiasis (VVC) is a common infection that affects an increasing proportion of women at childbearing age [1,2]. It is estimated that about 75% of healthy women have had at least one episode of VVC in her life and 40-50% have experienced recurrences [1,3]. The development of VVC depends on fungal factors related to Candida strains and host related factors [4].
The estrogenization of the vagina would be essential for colonization [5] . Colonization by Candida spp. is lower in girls before menarche and also in postmenopausal women, who usually do not suffer from VVC [4]. Vaginal colonization is higher in women with estrogenic vaginas, especially during pregnancy, so women who are colonized by Candida have a risk up to 35% of developing vaginitis after antibiotic treatment [4,6]. Other factors that have been studied are alterations of Lactobacillus biota, diabetes, genetic factors, use of contraceptives, corticosteroids, personal hygiene, type of clothing, atopic dermatitis and psycho - social stress that may cause immunosuppression [1,4,7].
Pregnancy is a predisposing factor due to high levels of glycogen and high hormonal load, so many women suffer multiple infections especially in the last trimester of pregnancy [8]. Similarly, the bearing of Candida spp., that in non-pregnant women is 10 to 17%, increases to 35% in pregnancy [9].
In general, it is considered that colonization is the first step towards vulvovaginitis whenever the patient has a predisposing factor, however the change from colonization to vaginitis is not well understood [4]. The epidemiological behavior of the genus Candida in the VVC used to be variable and it will depend on the level of estrogens in the vagina, immunosuppression or chronicity of the process [4].
This is the first research in pregnant women from Cartagena de Indias, north of Colombia, in which the main objective was identifying the vaginal colonizing Candida species and VVC species and specific objectives were identifying predisposing factors and susceptibility against fluconazole.
Materials and methods
Definition of the study population. The descriptive research was conducted in a total group of 76 pregnant women with vulvovaginitis symptoms (burning, itching, swelling, vaginal discharge, dyspareunia, odor) who were attending the external gynecological consultation at Clinica Maternidad Rafael Calvo (Maternal Clinic Rafael Calvo) in Cartagena de Indias (Colombia), from June to December 2014. Exclusion criteria included: no pregnancy, be younger than 16 years old, and vaginal bleeding. Comorbidities questionnaire for the study population was made according to scientific literature [1,8,10,11] .
Sampling: Patients were explained in detail about the objectives, the sampling and the relevance of the study. Patients agreed to sign informed consent, freely and without any financial compensation. The patient samples were taken by medical specialist in gynecology, using a swab and a speculum according to referenced by García-Heredia et al. [9]. Two swabs were taken; one spread on two slides and the other was placed in sterile sodium chloride solution (0.9%). Slides were properly transported in the shortest possible time to the Mycology Laboratory of the School of Medicine at Cartagena University.
Sample processing. Samples were processed for direct examination, Gram and Giemsa stains to evaluate the presence of fungal, bacterial and parasitic structures, inflammatory cells, and clue cells, pH measurement and Whiff test [12,13]. The criteria used to describe the vaginal biota were as follows: normal: when Lactobacillus spp. was predominant and almost no other morphotype were present; intermediate: when Lactobacillus morphotype are scarce and others may be scarcely observed; and association with infectious process: when predominated bacterial, yeast or parasites morphotype and Lactobacillus were not observed [14,15]. Amsel’s criteria for the diagnosis of bacterial vaginosis were used. These criteria include the presence of a homogeneous vaginal discharge; positive Whiff test, vaginal pH > 4.5 and observation of “Clue cells” in the direct examination of vaginal smears (12). The diagnosis of VVC was established according to the observation of blastoconidia, pseudohyphae or hyphae on direct examination of vaginal discharge and also positive culture of the sample [8,16]. It was identified as colonizing Candida spp. when the direct examination was negative and the culture was positive [8,16]. Bacterial vaginosis and candidiasis diagnosed in the same patient were classified as mixed infections.
Isolation and identification. The sample was cultured directly in CHROMagar® Candida (CHROMagar, France) and incubated at 37 °C for 24 to 48 hours [10] . Candida species were identified preliminary according to the colors produced by the colonies on CHROMagar Candida [17]; green isolates: Candida albicans, Candida dubliniensis, Candida africana; blue isolates: Candida tropicalis; dry pink: Candida krusei; creamy pink-lilac isolates: suspect of Candida glabrata, Candida parapsilosis, Candida guilliermondii; White isolates: other Candida spp.
Isolates were cultured on Sabouraud 4% glucose (SDA) without chloramphenicol (Merck, Germany) and then they were preserved in 30% glycerol at -72 °C. Clinical isolates and control strains used in phenotypic tests, susceptibility evaluation and multiplex PCR were cultured on SDA and incubated at 37 °C during 24 hours. Control strains were as follows: Candida albicans ATCC 90028, Candida tropicalis ATCC 750, Candida parapsilosis ATCC 22019, Candida glabrata ATCC 64677, Issatchenkia orientalis (Candida krusei) ATCC 6258, Candida lusitaniae ATCC 34449, Candida guilliermondii ATCC 6260, Candida dubliniensis GM0314.
The following tests for phenotypic differentiation of green isolates were carried out: Germ tube formation test in plasma [18], chlamydospores production in milk agar, macro and micro morphology in tobacco agar and growth at 45 °C according to Pineda et al. [19]. Conventional yeast fermentation test was also carried out [20,21] .
Multiplex PCR. Candida spp. DNA was obtained by Heat Shock Method proposed by Millar [22] , without enzymes. Multiplex PCR method used for amplification of Candida species was described by Carvalho et al. [23] . Universal primers UNI1 and UNI2 and species-specific primers: Calb, Cgla, Ckru, Cpar, Ctro, Cgui y Cdub, (Eurofins Mwg Operon; U.S.A), were also evaluated by Primer blast in http://www.ncbi.nlm.nih.gov/tools/primer-blast/. Multiplex PCR was developed according to Carvalho et al. [23] but with a final volume of 25 µl and using Kit GoTaq green Master Mix (Promega, USA). Final concentrations were used according to Carvalho et al. [23]. PCR reaction was ran in Perkin-Elmer GeneAmp PCR System 2400 (Perkin-Elmer, USA), as follows: an initial period of denaturation and enzyme activation for 10 min at 94 °C, 40 cycles of 15 seconds at 94 °C, 30 seconds at 55 °C and 45 seconds at 65 °C. The agarose gel was used at 2% for the electrophoretic run in TBE buffer (Tris-Borate-EDTA) plus ethidium bromide (5 µl/100 ml agarose). It was used Thermo Scientific GeneRuler 50bp DNA Ladder (Thermo Scientific, Lithuania). The run was performed in TBE buffer and at a voltage of 100 V. Pictures were recorded with Ingenius 3 Genesys version 1.2.7.0 Data Base Version 1.66 (Syngene, UK), 3.0 MP Camera (Synoptis, Japan).
Susceptibility evaluation to fluconazol. Antifungal susceptibility was assessed in triplicate by the method of broth microdilution minimal inhibitory concentration according to M27-A3 and M27-S4 documents of CLSI (Clinical and Laboratory Standards Institute) [24,25].
Preparation of the microplates with the antifungal Fluconazole stock solution (Sigma USA) was prepared with deionized sterile water at a concentration of 5120 mg /ml. The drug was then diluted in RPMI 1640 (Gybco, USA) plus MOPS (Sharlau, Spain). One hundred microliters of the final concentrations that ranged from 0.25 to 128 µg/ml were dispensed from columns 1 to 10 in sterile microplates (Nunclon Delta Thermo Scientific Surface, Denmark) 96 U-bottom wells. Column 11 was used to control growth and column 12 for the sterility control.
Inoculum preparation: Antifungal activity on clinical strains; Candida albicans, Candida tropicalis, Candida parapsilosis, Candida glabrata and control strains Candida parapsilosis ATCC 22019 and Issatchenkia orientalis (Candida krusei) ATCC 6258 were evaluated. The inoculum was adjusted visually according to a standard 0.5 McFarland scale (about 1x 106 to 5 x 106 CFU/ml) and then diluted 1:1000 in RPMI medium.
Microplates were incubated at 35-37 °C for 48 hours. The reading of the results was performed using an inverted mirror. Reading fluconazole was performed with a 50% inhibition compared to the growth control. The interpretation of the results was performed as susceptible, dose-dependent or resistant according to the cut-offs established in the M27-S4 supplement CLSI [24,25].
Results analysis: Frequencies and dispersion values, central trend and statistical significance for sociodemographic variables, symptoms, predisposing factors, phenotypic and molecular methods used were analyzed. The frequencies of predisposing factors and pathogenic colonizing species identified, and the results of the susceptibility tests were studied using the statistical program SPSS version 19.0 for Windows. [1].
Control of biases: The possible biases that could be presented correspond to information biases. However, the importance of providing reliable data was explained to the patients so that the results of the research will not be affected.
Ethical considerations: Patient data was preserved. All the patients were duly explained about the scope of the work and its benefits. Likewise, all the patients signed the informed consent.
Results
A total of 76 pregnant patients with symptoms associated with vulvovaginitis, prior informed consent freely signed, participated in the study conducted from June to December 2014. Most patients (63.2%) came from the provincial capital, Cartagena de Indias, while the rest of them lived on islands, municipalities and surrounding districts. Thirty five (46.1% completed high school 11 years of total education), but only 7 had continued with technical or professional studies. One important fact to note is that 90.8% of patients were engaged in household chores and were not independent economically (Table 1). It was determined the number of children as follows; 0 (28.9%), 1 (39.5%), 2 (18.4%), 3 (10.5%) and 4 (2.6%). It was established that 64.5% of patient were in third pregnancy trimester (29-40 weeks), 27.6% in second trimester (13-28 weeks) and 7.9% in first trimester (1-12 weeks).
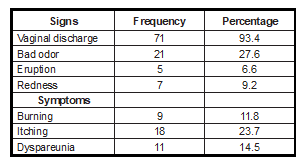
Predominant symptoms and signs of patients were vaginal discharge, followed by bad odor and itching, whereas the less frequent was vulvovaginal rash (Table 2).
Table 1. Sociodemographic data n = 76. * The remaining percentage did not answer the question. ** Waitress, Saleswoman. Source: authors.
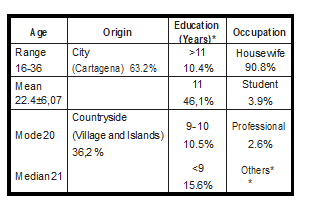
Table 2. Frequencies and percentages of signs and symptoms vulvovaginal. Source: authors.
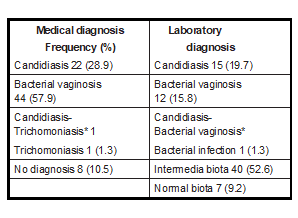
The medical diagnosis with the highest percentage (57.9%) was bacterial vaginosis which did not correspond with laboratory data, that according to Amsel criteria, only 15.8% 1had a diagnosis of bacterial vaginosis; however there was a better match with vaginal candidiasis diagnosis in terms of percentage. Laboratory results showed that intermediate biota dominated (52.6%) and it was not demonstrated, by direct examination or Giemsa staining the presence of T. vaginalis. While medical diagnosis bragged one Candida and Trichomonas mixed infection, on direct examination only candidiasis associated with bacterial vaginosis was evidenced. (Table 3).
The cultures of vaginal samples were positive in 54 (71.1%) patients, with a total of 56 isolates due to the growth of two species in the same sample in two cases. Growth in CHROMagar Candida isolates revealed 36 green, 7 pink, 5 blue, 5 white and 3 mauve.
Table 3. Comparative clinical diagnosis and laboratory results. * Mixed infections. Source: authors.
Green colonies were evaluated phenotypically in 36 isolates for preliminary differentiation of C. albicans, C. dubliniensis y C. africana. Germ tube test negative may occur for some strains of Candida albicans and Candida dubliniensis. The test at 45 °C preliminary identify 11 strains as C. dubliniensis. Tobacco agar test and Milk agar were more accuracy to identify C. albicans and C. dubliniensis according to results of the multiplex PCR Candida albicans corresponded to 34 green isolates and C. dubliniensis to 2 green isolates (Figure 1).
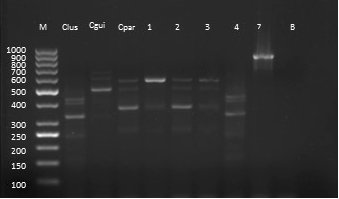
Figure 1. Green isolates multiplex PCR. M; DNA ladder bp, Calb; Candida albicans ATCC 90028; lane 1-6; Clinical strains, B; blank. Source: authors.
Pink, mauve and white isolates were evaluated by multiplex PCR (Figure. 2). As to the correspondence between CHROMagar Candida and multiplex PCR, it was found that the pink colonies could correspond to Candida krusei and Candida parapsilosis and that in regarding blue colonies, one was not identified as Candida tropicalis. Also some isolates could not be identified by multiplex PCR, because it only identifies eight species with the primers employed in this study.
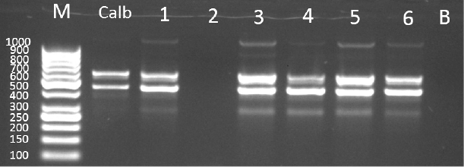
Figure 2. Multiplex PCR White and pink isolates. M: DNA ladder bp, Clus: Candida lusitaniae ATCC 34449, Cgui: Candida guilliermondii ATCC 6260, Cpar: Candida parapsilosis ATCC 22019, lanes 1-7; clinical strains, B; blank. 2and 3; Candida parapsilosis, 4; Candida lusitaniae. Source: authors.
The consensus among phenotypic testing and molecular test allowed the identification of species and determine the frequency of its presentation at the entire population and according to its role as a colonizing or pathogenic (Table 4).
Frequency of colonization by Candida was 71.4%. The most frequently isolated species was C. albicans followed in smaller proportion by C. tropicalis and Candida spp. This genus played a role as a pathogen in 28.6% of the study population, remaining C. albicans as the most frequently isolated, however the variation of species in VCC was lower than in colonized women. The frequency of risk factors related to the pathogenic or colonizing role of isolated yeasts is shown in Table 5.
Table 4. Frequency and percentages of the identified species, n=56. Source: authors.
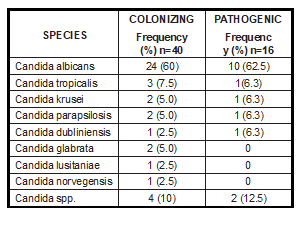
Table 5. Frequency of risk factors in colonizing Candida spp. and in VVC. Source: authors.
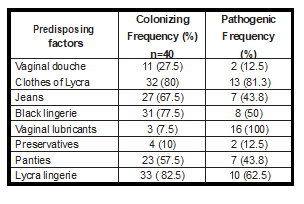
In patients colonized with Candida species were more frequent use of Lycra underwear, black Lycra outwear and jeans. In patients with vaginal candidiasis, all used vaginal lubricants and other common factor was the use of outer and interior Lycra clothing. In both groups the frequency of use of panties was similar. It should be noted that the patients had no other risk factors like treatment with broad-spectrum antibiotics or steroids, diabetes, innate or acquired immunosuppression or different from those described.
Isolates evaluated by the M27-A3 antifungal susceptibility method were all susceptible to fluconazole except two C. tropicalis resulting one as SSD (susceptible dose dependent) and the other resistant. Candida krusei strains are assumed to be intrinsically resistant.
Discussion
This descriptive study was conducted in 76 pregnant women attending gynecological outpatient maternity clinic in Cartagena de Indias city. The age range was between 16 to 36 years, mostly with a secondary education and dedicated to housework. Forty nine (64.5%) patients were in the last trimester of pregnancy and near 40% had one child. The most common symptom was vaginal discharge, followed by odor and itching. In the study by Rivero et al. [26] in pregnant patients from Venezuela, the predominant symptoms were also vaginal discharge (65% of cases) followed by itching. As for the correspondence between clinical and laboratory diagnosis, it was noted that bacterial vaginosis was the predominant clinical diagnosis in contrast to the finding of intermediate biota in the laboratory as the most frequent, so observation alone of symptoms does not allow to an accurate diagnosis in most cases, as well as noted Rathod et al., in a study of vulvovaginitis conducted in India, hence the importance of applying the relevant tests for a correct diagnosis [16]. It should be noted that it is a common practice in the population the self-medication and non-medical consultation due to the failure to regulate the sale of drugs, also the use of alternative treatments in search of improvement of symptoms, which can affect the low number of patients in gynecological consultation for vulvovaginal symptoms. The cultures of vaginal swabs were positive for 71.1% of the population (54 pregnant women), with a total of 56 isolates. In a similar study in India, Rathod et al. [16], found only 35% of positive cultures. In another study in pregnant women in Argentina [9], 28% of the cultures were positive and in Colombia, a study in Medellin also in pregnant women, prevalence was 33.3% [8]. The high percentage found in this investigation may be related to own environmental, dietary or physiological factors of pregnancy. 58.9% of the isolates were identified as Candida albicans, followed by Candida tropicalis (8.9%), Candida krusei (5.4%), Candida parapsilosis (5.4%) and other Candida species. Garcia-Heredia et al.(9) found, Candida albicans (90.4%) as the most prevalent species followed by Candida glabrata, Candida parapsilosis y Candia kefyr in VVC of pregnant women in Argentina. Duque et al. [8] in Medellín (Colombia) reported that Candida albicans (77%) was the most frequently isolated, followed by C. parapsilosis and C. tropicalis. The present study is consistent with the general literature on the most frequently isolated species, although variations occur with respect to other isolated species. The percentage of Candida colonization was 71.4%, which means isolates from women with no vaginal candidiasis. Only 28.6% of the study population presented vaginal candidiasis. The prevalence of vaginal candidiasis ranged from 9.5% according to Rathod et al. [16] and Andrioli et al [10] reported 47.9%. Among the important risk factors for colonization were more frequent those related to both outerwear and interior clothing materials, heat; while for women with vaginal candidiasis the most common was the use of vaginal lubricants. In the study by Andrioli et al. [10] in Brazil clothing was one of the distinguishing aspects in the groups studied. The isolates were susceptible to fluconazole, the most commonly used antifungal. Duque et al [8] similarly reported susceptibility to fluconazole for all isolates, although they used ATB fungus®. The frequency of Candida colonization in their population was relatively high 50%. VVC diagnosis was established only in 21.1% of the studied group.
The interpretation of symptoms and signs of the patients are not enough for the correct diagnosis of vulvovaginitis because there is not a high concordance between the diagnosis made by the physician and the results of clinical laboratory tests. In this study there was intermediate biota in many cases. Colonization by Candida species was more common in patients using clothing made from materials that generate heat, while in patients with VVC the most common factor was the use of vaginal lubricants and most strains tested were susceptible to fluconazole.
Acknowledgements.
María de la Vega for their technical support, to Maternal Clinic Rafael Calvo, to School of Medicine, Cartagena University, to Master of Medical Mycology, National Northern East University, Argentina.
Conflict of interest: the authors declare no conflict of interest.
Financiation: Cartagena University, Cartagena University Research Unit.
Literature cited
- Amouri I, Sellami H, Borji N, Abbes S, Sellami A, Cheikhrouhou F, et al. Epidemiological survey of vulvovaginal candidosis in Sfax, Tunisia. Mycoses 2010; 54:e499–e505 DOI: 10.1111/j.1439- 0507.2010.01965.x.
- Fischer G, Bradford J. Vulvovaginal candidiasis in postmenopausal women: the role of hormone replacement therapy. J Low Genit Tract Dis 2011; 15(4):263-7. DOI: 10.1097/LGT.0b013e3182241f1a.
- Sobel JD. Recurrent vulvovaginal candidiasis. Am J Obstet Gynecol 2016; 214(1):15-21. DOI: 10.1056/ NEJM198612043152305.
- Mendling W, Brasch J. Guideline vulvovaginal candi- dosis (2010) of the german society for gynecology and obstetrics, the working group for infections and infectimmunology in gynecology and obstet- rics, the german society of dermatology, the board of german dermatologists and the german speak- ing mycological society. Mycoses 2012; 55(Suppl. 3):1-13. DOI: 10.1111/j.1439-0507.2012.02185.x.
- Tarry W, Fisher M, Shen S, Mawhinney M. Candida albicans: the estrogen target for vaginal colo- nization. J Surg Res 2005; 129(2):278-82. DOI: 10.1016/j.jss.2005.05.019.
- Pirotta MV, Garland SM. Genital Candida species detected in samples from women in Melbourne, Australia, before and after treatment with anti- biotics. J Clin Microbiol 2006; 44(9):3213-7. DOI: 10.1128/JCM.00218-06.
- Goncalves B, Ferreira C, Alves CT, Henriques M, Azeredo J, Silva S. Vulvovaginal candidiasis: Epidemiology, microbiology and risk factors. Critical reviews in microbiology 2015; 21:1-23. DOI: 10.3109/1040841X.2015.1091805
- Duque C, Uribe OL, Soto AF, Alarcon JR. Candidiasis vulvovaginal en un grupo de mujeres gestantes de Medellin, Colombia. Infectio 2009; 13(1):14-20. DOI:https://doi.org/10.1016/S0123-9392(09)70139-0.
- Garcia-Heredia M, Garcia SD, Copolillo EF, Cora- Eliseth M, Barata AD, Vay CA, et al. [Prevalence of vaginal candidiasis in pregnant women. Identifi- cation of easts and susceptibility to antifungal agents]. Rev Argent Microbiol 2006; 38(1):9-12.
- Andrioli JL, Oliveira GS, Barreto CS, Sousa ZL, Oli- veira MC, Cazorla IM, et al. Frequency of yeasts in vaginal fluid of women with and without clinical suspicion of vulvovaginal candidiasis. Rev Bras Ginecol Obstet 2009; 31(6):300-4. DOI: http://dx.doi. org/10.1590/S0100-72032009000600006.
- Guzel AB, Ilkit M, Akar T, Burgut R, Demir SC. Evaluation of risk factors in patients with vul- vovaginal candidiasis and the value of chromID Candida agar versus CHROMagar Candida for recovery and presumptive identification of vaginal yeast species. Med Mycol 2010; 49(1):16-25. DOI: 10.3109/13693786.2010.497972.
- Vera LM, López, N, Arámbula AL. Validez y repro- ducibilidad del sistema de puntuación de Nugent para el diagnóstico de vaginosis bacterianas en mujeres embarazadas. Rev Chil Obstet Ginecol 2009; 75(5):286-91.DOI: http://dx.doi.org/10.4067/ S0717-75262009000500004.
- Buscemi L, Arechavala A, Negroni R. Estudio de las vulvovaginitis agudas en pacientes adultas, sexualmente activas, con especial referencia a la candidiasis, en pacientes del hospital de in- fecciosas Francisco J. Muñiz. Rev Iberoam Micol 2004; 21:177-81.
- Alves DC, Cassamassimo MT, Da Silva MG, Garcia de Lima CM. Alteración de la flora vaginal en gestantes de bajo riesgo atendidas en servicio público de salud: prevalencia y asociación a la sintomatología y hallazgos del examen ginecoló- gico. Rev Latino-Am Emfermagem 2010; 18(5):1-9.
- Hiller SL, Krohn MA, Nugent RP, Gibbs RS. Charac- teristics of three vaginal flora patterns assessed by gram stain among pregnant women. Vaginal Infections and Prematurity Study Group. Am JObstet Gynecol 1992; 166(3):938-44.
- Rathod SD, Klausner JD, Krupp K, Reingold AL, Madhivanan P. Epidemiologic features of Vul- vovaginal Candidiasis among reproductive-age women in India. Infect Dis Obstet Gynecol 2012; 2012:859071. DOI: https://doi.org/10.1016/0002- 9378(92)91368-K.
- Odds FC, Bernaerts R. CHROMagar Candida, a new differential isolation medium for presump- tive identification of clinically important Candida species. J Clin Microbiol 1994; 32(8):1923-9.
- Duarte A, Marquez A, Araujo C, Perez C. Modali- dades de la prueba de tubo germinal. Rev Soc Ven Microb 2009; 29:66-8.
- Pineda G, Scollo K, Santiso G, Lehmann E, Arecha- vala A. Aislamiento de Candida dubliniensis en distintos materiales clínicos. Análisis de méto- dos fenotípicos de diferenciación con Candida albicans. Rev Argen Microb 2008; 40:211-17.
- Pincus DH, Orenga S, Chatellier S. Yeast iden- tification--past, present, and future meth- ods. Med Mycol 2007; 45(2):97-121. DOI : 10.1080/13693780601059936.
- Kali A, Srirangaraj S, Charles PM. A cost-effective carbohydrate fermentation test for yeast using microtitre plate. Indian j Medical Microbiol 2015; 33(2):293-5. DOI: 10.4103/0255-0857.154884.
- Millar BC, Jiru X, Moore JE, Earle JA. A simple and sensitive method to extract bacterial, yeast and fungal DNA from blood culture material. J Mi- crobiol Methods 2000; 42(2):139-47. DOI: 10.1016/ S0167-7012(00)00174-3.
- Carvalho A, Costa-De-Oliveira S, Martins M L, Pi- na-Vaz C, Rodrigues AG, Ludovico P, Rodrigues F. Multiplex PCR identification of eight clinically relevant Candida species. Med Mycol 2007; 45(7):619-27. DOI: 10.1080/13693780701501787.
- Clinical and Laboratory Standards Committe Insti- tute. Reference Method for Broth Dilution Anti- fungal Susceptibility Test of Yeasts, Approved Standard- Third edition. Wayne: Clinical and Laboratory Standards Committe Institute; 2008.
- Clinical and Laboratory Standards Committe Institute. Reference Method for Broth Dilution Antifungal Susceptibility Testing of Yeasts; Fourth Informa- tional Supplement. Wayne: Clinical and Laboratory Standards Committe Institute; 2012.
- Rivero M, Diaz J, Centeno S. Frecuencia de espe- cies de Candida aisladas en pacientes embara- zadas con vulvovaginitis. Rev Soc Ven Microbiol 2003; 3(2):148-152.
